
Comment:
The traditional cardiological focus on lowering LDL-C in the elderly rests on a foundation of biochemical plausibility that is increasingly dismantled by actual survival data. This systematic review identified a critical physiological disconnect: for those over age 60, high LDL-C is not a mortality stressor but is actually associated with a longer lifespan. In 92% of the participants where an association was found, higher LDL-C correlated with a lower risk of all-cause mortality. We must stop viewing lipids through the narrow lens of atherogenesis and start recognizing their role in maintaining structural integrity and immune resilience.
The hierarchy of harm in this cohort is unambiguous. While the conventional standard-of-care prioritizes the pharmacological reduction of LDL-C, the hard clinical endpoint of overall survival favors those with higher levels. Specifically, the data suggests that LDL-C serves as an efficacious buffer against infections and cancer, two of the primary survival hazards in an aging population. The definitive takeaway for the clinician is that for patients over 60, high LDL-C is a marker of biological robustness rather than disease. We must re-evaluate guidelines that promote the suppression of this vital prohormone substrate, as achieving lower levels may paradoxically increase the risk of a shorter lifespan.
Summary:
Clinical Bottom Line
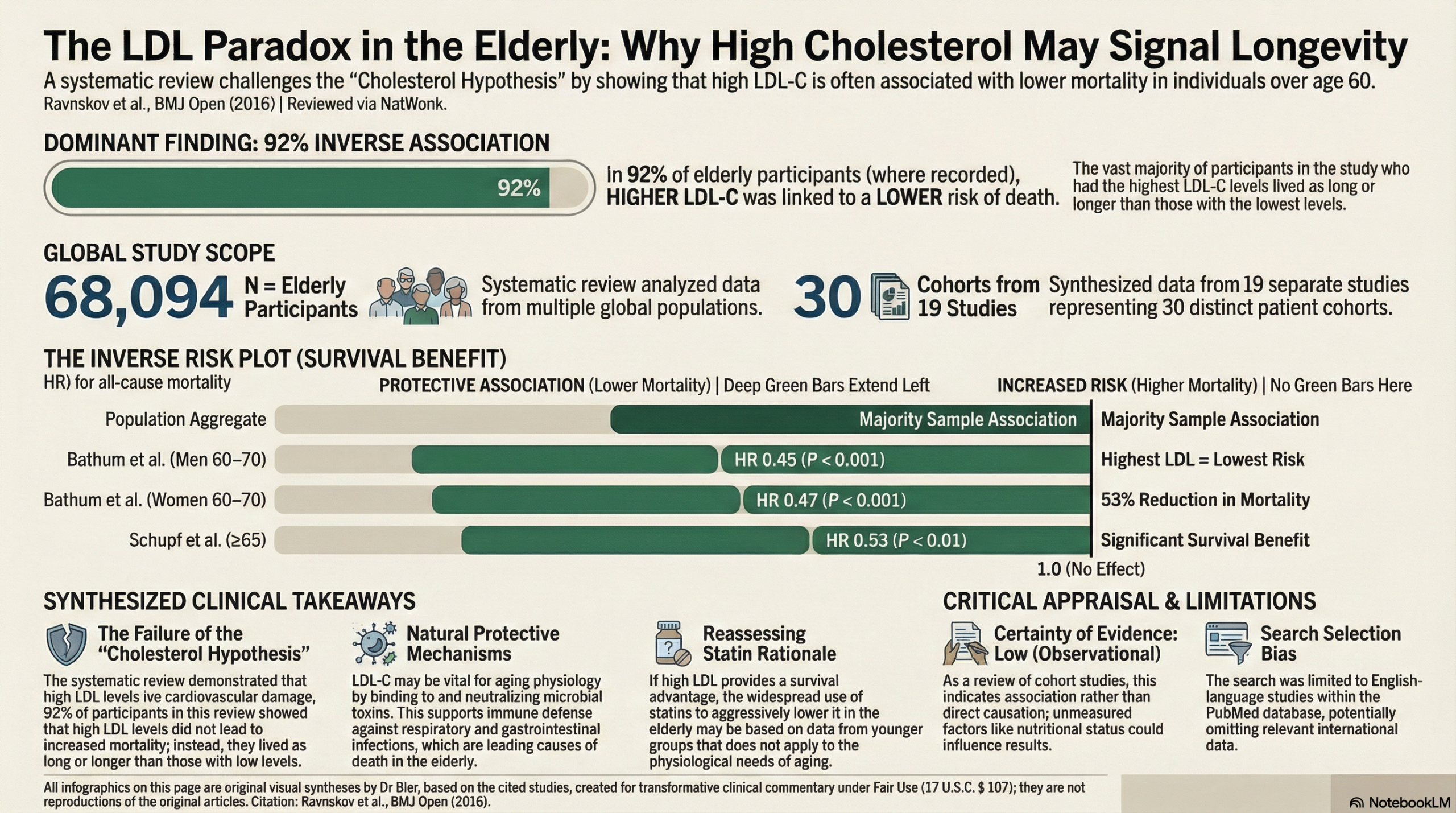
This systematic review presents a provocative challenge to the conventional cholesterol hypothesis. In an analysis of cohort studies including over 68,000 individuals older than 60, high low-density lipoprotein cholesterol (LDL-C) was not associated with increased mortality. In fact, for the vast majority of participants (92%), higher LDL-C was associated with a lower risk of death. These findings suggest that for elderly patients, high LDL-C may not be a risk factor for mortality and could potentially be protective, a conclusion that directly contradicts current cardiovascular disease prevention guidelines.
Results
Summary of Results
The review identified 19 cohort studies that evaluated the association between LDL-C and mortality in people aged 60 and older.
-
All-Cause Mortality: This outcome was assessed in 28 distinct cohorts. In 16 of these cohorts, representing 62,740 of the 68,094 total participants (92%), there was an inverse association between LDL-C and all-cause mortality, meaning individuals with higher LDL-C levels lived as long or longer than those with low LDL-C. In the remaining cohorts, no association was found.
-
Cardiovascular (CV) Mortality: This was reported in nine cohorts. In two of these, mortality was highest in the group with the lowest LDL-C. In the other seven cohorts, there was no association between LDL-C and CV mortality.
The authors propose potential mechanisms for this unexpected protective association, suggesting high LDL-C may play a role in protecting against infections and cancer. They cite evidence that LDL can bind to and inactivate microorganisms and that low cholesterol has been linked to a higher risk of hospitalization for infectious diseases and higher mortality from respiratory and gastrointestinal diseases.
Assertive Critical Appraisal
-
Certainty of Evidence (GRADE Framework): The certainty of this evidence should be considered Low. This is a review of observational cohort studies, which cannot prove causation. The conclusions are weakened by significant methodological limitations of the review itself, including a search strategy restricted to a single database (PubMed) and only English-language papers, which increases the risk of missing relevant studies.
-
Heterogeneity: The authors do not report a statistical measure of heterogeneity (like the $I^2$ statistic). While they describe the different findings across studies (some inverse association, some no association), the lack of a quantitative assessment makes it difficult to judge whether pooling these results would even be appropriate and how consistent the effect truly is.
-
Publication Bias: The authors did not perform a formal assessment for publication bias, such as a funnel plot. They acknowledge that their search strategy may have missed studies where LDL-C and mortality were analyzed but not mentioned in the abstract or title, creating a potential for selection bias.
-
Risk of Bias in Included Studies: The primary concern in the underlying cohort studies is “inverse causation”—the possibility that pre-existing serious illness causes low cholesterol rather than low cholesterol causing mortality. The authors attempt to rebut this by highlighting that the inverse association between LDL-C and mortality remained significant even in three large studies that excluded participants with terminal illness or those who died within the first year.
-
Reporting Quality Assessment (PRISMA): The review includes a PRISMA-style flow diagram showing the study selection process. However, the failure to describe a comprehensive search strategy across multiple databases and the lack of a formal risk of bias assessment for each included study are significant reporting omissions that reduce the review’s transparency and reliability.
Research Objective
To systematically review the available literature to investigate whether LDL-C is a risk factor for all-cause and/or cardiovascular (CV) mortality in individuals from the general population aged 60 years or older.
Study Design
This is a systematic review of published cohort studies. The authors searched the PubMed database for relevant studies published in English. They included studies of people aged ≥60 years from the general population where LDL-C was measured at baseline and all-cause or CV mortality was reported at follow-up.
Setting and Participants
The review included a total of 68,094 individuals from 19 separate studies (representing 30 cohorts). All participants were aged 60 years or older at the start of their respective studies.
Bibliographic Data
-
Title: Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review
-
Authors: Uffe Ravnskov, David M Diamond, Rokura Hama, et al.
-
Journal: BMJ Open
-
Year: 2016
Original Article:
Full text – Pubmed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.