
Comment:
It is always tempting when an elegant preclinical mechanism is paired with human level data. However, we have to be incredibly careful when translating these findings.
The Preclinical Mechanism vs. The Non-Alzheimer’s Signal
On the basic science side, the authors present a compelling piece of spatial biology, demonstrating that transgenic Alzheimer’s disease (AD) mouse models exhibit a conserved phenotype of brain hyperglycosylation. When they flooded the hexosamine biosynthetic pathway of these AD-vulnerable mice with oral glucosamine, it accelerated their cognitive decline—suggesting that adding substrate to an already burning pathological fire can worsen outcomes.
However, the most critical piece of data in the animal models—and the one that will likely be overlooked by sensationalist headlines—is how glucosamine affected the wild-type (WT) control mice. When the researchers subjected cognitively normal, non-Alzheimer’s mice to the exact same glucosamine regimen, the results were entirely flat. There was no increase in brain glycan abundance and absolutely no cognitive impairment.
The normal brain clearly possesses robust, intrinsic metabolic resilience that easily buffers against this substrate influx. This distinction is vital for our clinical interpretation: even if the mouse model is entirely accurate (which we know mice models rarely are), it proves that glucosamine does not cause or increase the baseline risk of initiating Alzheimer’s pathology in a healthy brain.
The Human EHR Mirage: Confounding by Indication
To complement the mouse data, the authors conducted a retrospective analysis of human electronic health records (EHR), reporting that over-the-counter glucosamine use among dementia patients was associated with accelerated disease progression and a 25% increase in mortality risk. On the surface, it seems like a perfect match for the animal data.
In reality, the human dataset suffers from a fatal epidemiological flaw: confounding by indication. While the authors did control for a wide array of standard demographic and metabolic variables in their statistical models, they failed to control for any underlying pain conditions or a diagnosis of arthritis. Glucosamine is not a random exposure; it is a surrogate marker for a patient suffering from chronic joint pain, osteoarthritis, or structural musculoskeletal degeneration.
By failing to isolate the supplement from the primary pathologies it treats, the model is almost certainly capturing the systemic impact of chronic pain and immobility rather than any biochemical harm from glucosamine itself. Chronic osteoarthritis represents a state of persistent, low-grade systemic inflammation, which is a well-documented driver of accelerated neurodegenerative decline. Furthermore, severe joint pain naturally limits physical activity in an aging population. A sudden drop in mobility is intimately tied to rapid cognitive decline, cardiovascular events, and worsened overall survival. The cohort taking glucosamine was inherently carrying a heavier baseline burden of pain and physical frailty than the non-user controls from the very start.
If a patient has an advanced, established neurodegenerative condition, a cautious suspension of glucosamine might be a reasonable, conservative step. However, for the general, cognitively intact population using it for joint preservation, there is no sound empirical or biological basis here to suggest a risk. When a retrospective human model accidentally attributes the systemic toll of chronic arthritis and physical immobility to the supplement treating it, we are looking at an observational artifact, not a clinical finding.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
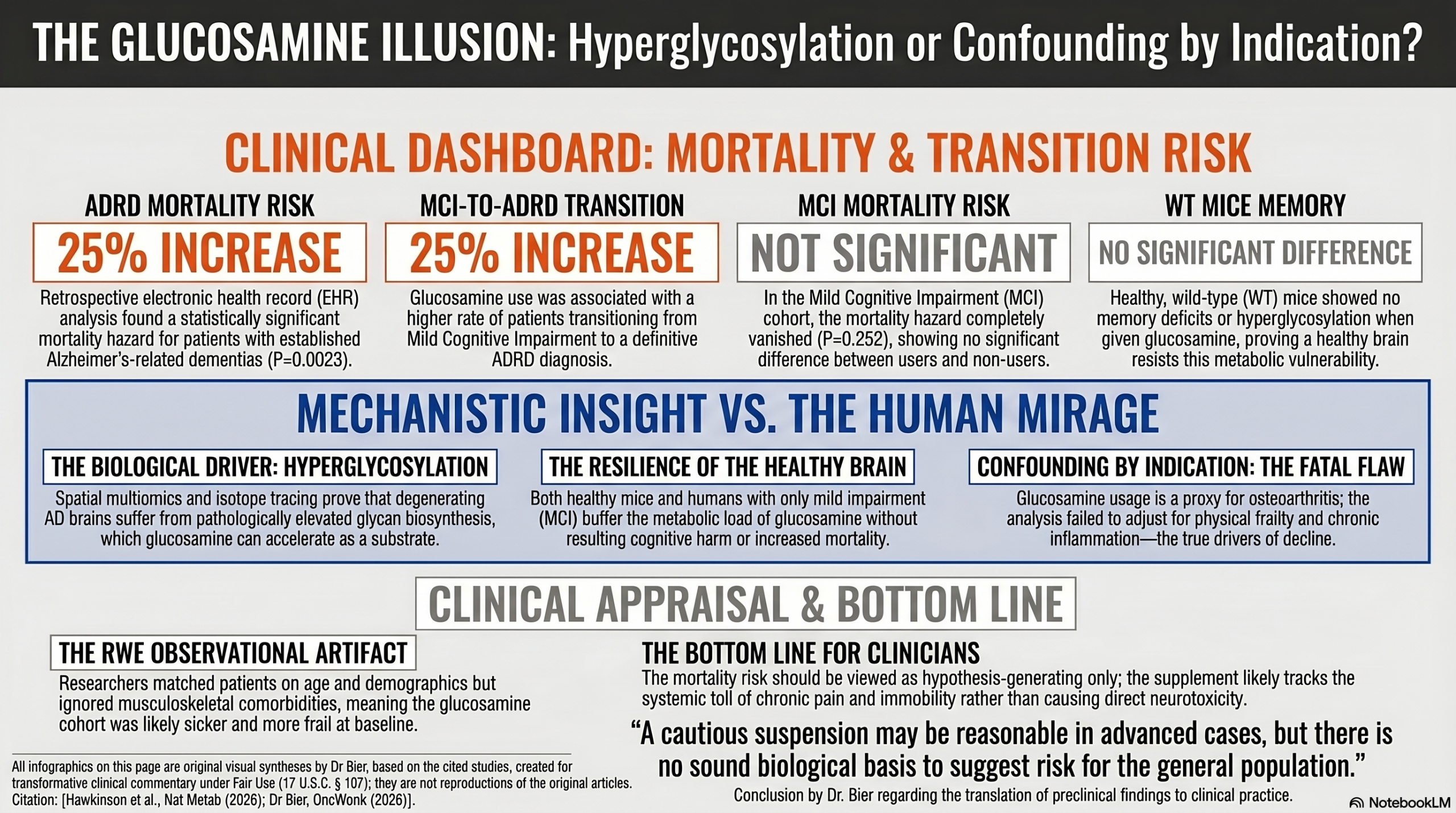
This cohort study (nested within a broader basic science paper) shows a strong association between glucosamine supplementation and an increased risk of mortality and disease progression in patients with Alzheimer’s disease-related dementias (ADRD). However, it is not possible to conclude that glucosamine biologically causes these worsened outcomes due to the profound potential for unmeasured confounding variables—specifically, “confounding by indication.” Glucosamine is an over-the-counter supplement taken for osteoarthritis and joint pain; therefore, the users of this supplement likely suffer from chronic pain and reduced physical mobility, both of which are independent, powerful drivers of cognitive decline and mortality.
The study’s basic science arm attempts to bypass this human confounding loop through controlled animal models. The authors demonstrated that daily oral glucosamine directly drove brain hyperglycosylation and exacerbated memory deficits in Alzheimer’s-model mice (5xFAD). In contrast, healthy wild-type mice completely buffered the supplement, showing zero metabolic or cognitive impairment. This suggests that while ‘confounding by indication’ heavily clouds the human real-world evidence, a degenerating brain may indeed possess a distinct, disease-specific metabolic vulnerability to glycan expansion that healthy tissue naturally resists.”
Results in Context
- Main Results: In the ADRD cohort, glucosamine usage was associated with a 25% increase in mortality risk ($P=0.0023$). In the Mild Cognitive Impairment (MCI) cohort, glucosamine usage did not significantly impact overall mortality, but it was associated with a 25% increase in the proportion of patients transitioning from MCI to a definitive ADRD diagnosis. The authors attempted to adjust for confounders using propensity score matching for age and demographic variables.
- Definitions: A 25% increase in mortality risk (or a hazard ratio of 1.25) means that the probability of death occurring at any given time during the study period was 1.25 times higher in the exposed group (glucosamine users) than in the unexposed group (non-users). Propensity score matching is a statistical technique used to balance measured characteristics (like age and sex) between the treatment and control groups to simulate a randomized environment.
- Participants: The survival analysis included a total of 24,481 patients with ADRD and 41,884 patients with MCI.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): The clinical real-world evidence (RWE) portion of this study is critically limited by “confounding by indication.” Glucosamine is heavily marketed and utilized as a joint health supplement. Patients taking glucosamine are fundamentally different from non-users because they actively suffer from joint-related conditions (e.g., osteoarthritis), which cause chronic pain and decreased physical activity. Reduced mobility, frailty, and chronic inflammation are all potent risk factors for early mortality and the acceleration of dementia. Because the authors matched patients strictly on age and demographic variables rather than underlying mobility status, pain scores, or osteoarthritis diagnoses, the observed “harm” from glucosamine may entirely reflect the worsened health status of the patients who need the supplement, rather than the biochemical effect of the supplement itself.
- Reporting Quality Assessment (STROBE): You must explicitly flag that while the authors clearly defined their matching criteria for age and demographics, they do not clearly describe efforts to address potential sources of clinical confounding (such as comorbid joint disease, baseline functional status, or frailty metrics). This is the most critical methodological challenge in observational research, and its omission here is a major flaw that threatens the internal validity of the clinical claim.
- Reporting Quality Assessment (RECORD) for RWE Studies: The study utilizes routinely collected health data from an electronic health record (EHR) system. The authors adequately define how participants were selected and how exposures were defined, noting the use of a natural language processing pipeline to extract glucosamine usage from physician notes. However, relying on unstructured clinical notes for over-the-counter supplement tracking carries a high risk of misclassification bias, as patients often fail to report non-prescription supplements to their physicians.
- Applicability: While the mechanistic, basic science portions of this paper provide compelling evidence regarding hyperglycosylation , the epidemiological findings regarding over-the-counter glucosamine cannot be confidently applied to general clinical practice. Until randomized controlled trials or strictly controlled observational studies (adjusting for musculoskeletal comorbidities) are performed, clinicians should view the association between glucosamine and AD progression as hypothesis-generating rather than definitive.
- Research Objective: To investigate whether glucosamine usage influences clinical outcomes, mortality, and disease progression in patients with AD and MCI.
- Study Design: Retrospective cohort study utilizing electronic health records.
- Setting and Participants: The study analyzed EHR data from 2012 to 2024 via the University of Florida Health Integrated Data Repository. Participants included patients with a documented diagnosis of MCI or AD/ADRD (including vascular, Lewy body, and frontotemporal dementia).
Bibliographic Data
- Title: Hyperglycosylation is a metabolic driver of Alzheimer’s disease
- Authors: Tara R. Hawkinson, Zizhen Liu, Roberto A. Ribas, et al.
- Journal: Nature Metabolism
- Year: 2026
- DOI: 10.1038/s42255-026-01538-4
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.