
Comment:
It seems logical to assume that if elevated cholesterol increases cardiovascular risk, it must damage all vascular beds equally—threatening the brain just as much as the heart. Furthermore, most assume that the extreme elevations seen in familial hypercholesterolemia (FH) must confer a universally catastrophic risk. This study proves those assumptions wrong.
This research serves as a robust rebuttal to the “universal toxin” theory of LDL. By utilizing Mendelian randomization, the authors reveal a critical hierarchy of harm: while genetically high LDL is indeed a causal factor for myocardial infarction, it is not an independent risk factor for ischemic stroke. The data demonstrates that FH patients are not at higher risk of stroke unless they have already developed ischemic heart disease. This distinction means that stroke risk in FH is not a direct consequence of cholesterol clogging cerebral arteries, but a secondary downstream effect of heart disease (likely via mural thrombi).
We have to not treat “CVD” as a single entity and recognize that high cholesterol in FH targets the heart, not the brain; protect the heart, and you protect the brain—but the reverse is not true.
Summary:
Clinical Bottom Line
This large-scale prospective cohort study and Mendelian randomization analysis found that familial hypercholesterolemia (FH) and high low-density lipoprotein (LDL) cholesterol are not independently associated with an increased risk of ischemic stroke. While certain clinical diagnostic criteria (specifically the Dutch Lipid Clinic Network) showed a higher stroke risk, this association was driven by a history of ischemic heart disease (IHD) rather than the elevated LDL cholesterol itself. These findings suggest that the primary clinical benefit of LDL-lowering therapy in FH patients is the reduction of myocardial infarction, with stroke prevention being a secondary consequence of preventing heart disease rather than a direct effect of lowering LDL.
Results in Context
Main Results
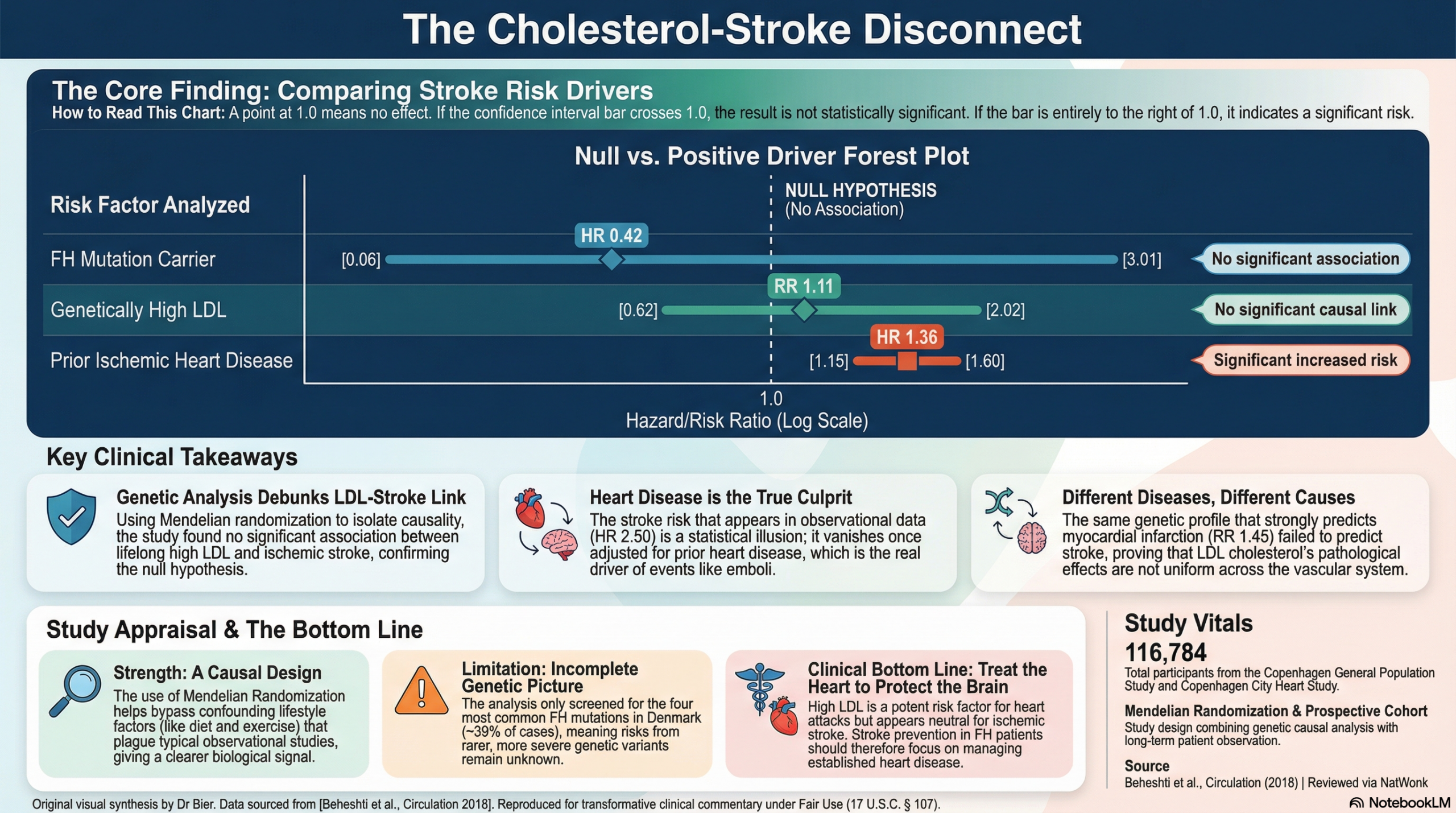
- Genetically Defined FH: There was no association between carrying FH causative mutations (LDLR or APOB) and the risk of ischemic stroke (multivariable-adjusted Hazard Ratio [HR]: 0.42; 95% CI, 0.06–3.01).
- Mendelian Randomization (Causal Analysis): For a 1 mmol/L higher LDL cholesterol concentration, the causal genetic risk ratio was 1.11 (0.62–2.02) for ischemic stroke, which was not statistically significant. In contrast, the same increase was significantly associated with myocardial infarction (risk ratio: 1.45; 1.08–1.93).
- Clinical FH Criteria: * Using Simon Broome or MEDPED criteria, no association was found with ischemic stroke.
- Using Dutch Lipid Clinic Network (DLCN) criteria, a 2.5-fold higher risk of stroke was initially observed (HR: 2.50; 1.33–4.69) for “definite or probable” FH.
- The Role of Ischemic Heart Disease (IHD): The higher stroke risk identified via DLCN criteria was only present in individuals who had IHD before baseline. IHD at baseline was independently associated with a higher stroke risk (HR: 1.36; 1.15–1.60).
Definitions
- Hazard Ratio (HR): A measure of how often an event happens in one group compared to another over time; for example, an HR of 1.36 indicates a 36% relative increase in the risk of stroke compared to the reference group.
- Mendelian Randomization: A method using genetic variants as proxies for environmental exposures (like LDL levels) to determine if an association is truly causal rather than just a correlation.
Participants
- The study analyzed 106,412 individuals from the Copenhagen General Population Study (CGPS) and 10,372 individuals from the Copenhagen City Heart Study (CCHS).
- For prospective analyses, 1,649 individuals were excluded due to prior stroke, leaving 104,763 individuals in the primary cohort.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Confounding: The authors adjusted for a wide range of factors including smoking, hypertension, and diabetes. However, they correctly note that residual confounding cannot be entirely excluded in observational analyses.
- Genetic Coverage: The study only screened for the four most common FH mutations in Denmark, accounting for approximately 39% of FH mutations in that population. It remains unclear if rarer, more deleterious mutations would alter the stroke risk profile.
- Potential Underdiagnosis: Clinical FH may have been underdiagnosed because the researchers lacked data on tendon xanthomas and arcus corneae, which are key components of standard clinical diagnostic criteria.
Reporting Quality Assessment (STROBE)
- The authors provided a detailed description of their efforts to address confounding by using multivariable adjustment and stratifying results by baseline IHD to isolate the effect of LDL cholesterol. This transparency allows for the critical observation that stroke risk in FH patients is likely mediated by cardiac complications (like mural thrombi from myocardial infarction) rather than direct atherosclerotic effects of LDL in the cerebral vasculature.
Applicability
- The study population consisted exclusively of white individuals of Danish descent. While there is no known biological reason these results would not apply to other ethnicities, the findings have not been formally validated in more diverse populations.
Research Objective
To test the hypothesis that individuals in the general population with familial hypercholesterolemia (FH) and/or high LDL cholesterol have a higher risk of ischemic stroke.
Study Design
A prospective cohort study utilizing both observational data and Mendelian randomization (causal genetic analysis) across two large independent populations.
Setting and Participants
- Setting: General population of Copenhagen, Denmark.
- Participants: 116,784 white adults followed for a median of up to 38 years through national Danish registries.
Bibliographic Data
- Title: Relationship of Familial Hypercholesterolemia and High Low-Density Lipoprotein Cholesterol to Ischemic Stroke
- Authors: Sabina Beheshti, Christian M. Madsen, Anette Varbo, Marianne Benn, Børge G. Nordestgaard
- Journal: Circulation
- Year: 2018
- DOI: 10.1161/CIRCULATIONAHA.118.033470
Original Article:
Full text: here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.