
Comment:
A central issue in sleep medicine is the conflict between the risk of not sleeping, and the risk of taking sedative-hypnotics to help sleep. Most people assume medication induced sleep is better than not sleeping.
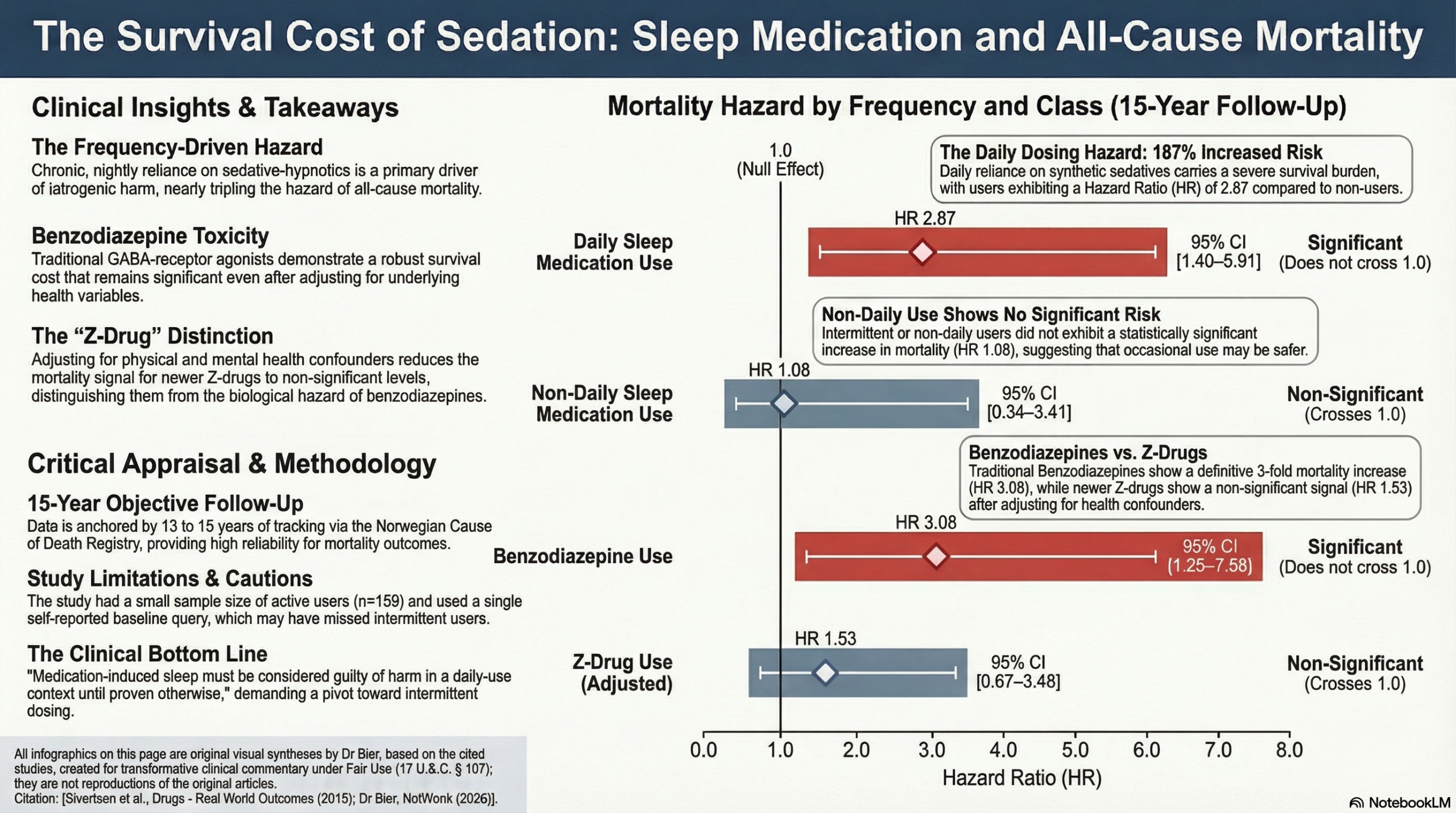
This 15-year prospective data confirms that daily usage is associated with nearly three times the hazard of death compared to non-users, though the limited sample size of 159 medication users necessitates a cautious interpretation of the exact risk magnitude. However, even with these wide confidence intervals, the discrepancy between benzodiazepines (HR 3.08) and the relatively neutral signal of Z-drugs (HR 1.53) suggests that not all sedative classes carry the same survival cost.
The tangible significance is that medications in this class must be considered guilty of harm in a daily-use context until proven otherwise. By acknowledging that the mortality signal is strongest for benzodiazepines and daily habits, we need to refine the approach to avoid the most hazardous patterns of use. Transitioning patients toward natural modulators and intermittent strategies remains the most survival-oriented path, especially when the long-term safety of synthetic alternatives remains statistically precarious.
Sleep Medication Classes and Common Examples
Benzodiazepines These are traditional sedative-hypnotics that act on the GABA receptor and were associated with a 3-fold increase in mortality risk in this study.
-
Diazepam (Valium)
-
Lorazepam (Ativan)
-
Alprazolam (Xanax)
-
Temazepam (Restoril)
-
Oxazepam (Serax)
Z-drugs (Non-benzodiazepine Hypnotics) These are newer medications designed to target specific subsets of GABA receptors, which showed a non-significant risk after adjusting for health factors in this cohort.
-
Zolpidem (Ambien)
-
Zopiclone (Imovane/Zimovane)
-
Esopiclone (Lunesta)
-
Zaleplon (Sonata)
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This prospective cohort study demonstrates a significant association between the use of sleep medications and increased all-cause mortality over a 13- to 15-year period. The risk is particularly pronounced for users of benzodiazepines (3-fold increased risk) and those reporting daily usage (nearly 3-fold increased risk). While the study identifies a strong association, its observational nature and the relatively small number of medication users mean it cannot prove that sleep medications directly cause death. The findings suggest clinicians should exercise caution when prescribing these agents, especially for long-term daily use.
Results in Context
Main Results
- Any Sleep Medication Use: Reported use was associated with a twofold increase in the risk of mortality in the fully adjusted model (HR 1.97; 95% CI 1.06–3.66).
- Frequency of Use: Daily users faced a significantly higher risk (HR 2.87; 95% CI 1.40–5.91) compared to non-users. Non-daily usage did not show a statistically significant increase in mortality risk (HR 1.08; 95% CI 0.34–3.41).
- Type of Medication: Benzodiazepine use was associated with a 3-fold risk (HR 3.08; 95% CI 1.25–7.58). While Z-drugs showed an increased risk in crude analyses, the association became non-significant after adjusting for health factors (HR 1.53; 95% CI 0.67–3.48).
Definitions
- Hazard Ratio (HR): A measure of how often a particular event (death) happens in one group compared to another over time. An HR of 2.87 means the daily user group had 2.87 times the “hazard” of death compared to the control group.
- 95% Confidence Interval (CI): A range of values that is likely to include the true effect size. If the range includes 1.0, the result is typically considered not statistically significant.
Participants
- The study initially invited 29,400 residents of Hordaland County, Norway.
- A total of 21,826 participants provided valid data and informed consent.
- Only 159 individuals (0.7%) reported using sleep medication on the day prior to baseline.
- During the 13–15 year follow-up, 622 (2.8%) participants died.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Exposure Misclassification: Exposure was based on a single question: “Did you take any medication yesterday?”. This likely captured chronic/heavy users but missed intermittent users who did not take a pill that specific night, potentially biasing results toward those with more severe insomnia or morbidity.
- Statistical Power: The small number of sleep medication users (n=159) resulted in wide confidence intervals, particularly for subgroup analyses (e.g., non-daily users), which reduces the precision of the risk estimates.
- Residual Confounding: While the authors adjusted for mental health, physical diagnoses, and pain, they could not fully account for the severity of the underlying insomnia itself21. It remains unclear if the medication or the sleep disorder (or associated comorbidities) is the primary driver of mortality.
Reporting Quality Assessment (STROBE & RECORD)
- STROBE Compliance: The authors clearly described their efforts to address confounding by utilizing multi-step Cox proportional hazards models, adjusting for sociodemographic factors, lifestyle, and health status.
- RECORD (Real-World Evidence): The study utilized the Norwegian Cause of Death Registry, a highly reliable national database. The methods for linking this registry to the HUSK study population were adequately described, enhancing the validity of the outcome measurement.
- Missing Data: The study lacked data on dosage, duration of use, or medication changes during the long follow-up period, which is a significant limitation for establishing a dose-response relationship.
Applicability
- The findings are highly relevant to community-dwelling middle-aged adults (born 1950–1957). However, the very low prevalence of reported use (0.7%) compared to national prescription registries (approx. 5.8%) suggests the study population may not perfectly represent the average sleep medication user in general clinical practice.
Research Objective
To examine the prospective association between the use of different types and frequencies of sleep medications and all-cause mortality.
Study Design
A prospective cohort study linking self-reported community health data (HUSK) to national death registry data with a 13- to 15-year follow-up.
Setting and Participants
- Setting: Hordaland County, Norway.
- Dates: Baseline data collected 1997–1999; mortality follow-up through December 2012.
- Inclusion: Community dwellers born between 1950–1951 and 1953–1957
Bibliographic Data
- Title: Use of Sleep Medications and Mortality: The Hordaland Health Study
- Authors: Børge Sivertsen, Ida E. H. Madsen, Paula Salo, Grethe S. Tell, Simon Øverland
- Journal: Drugs – Real World Outcomes
- Year: 2015
- DOI: 10.1007/s40801-015-0023-8
Original Article:
Full text pdf: here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.