
Comment:
I incorporate high-sensitivity CRP into every cardiovascular workup because it captures a physiological reality that standard lipid panels miss. As this foundational paper details, hsCRP identifies high-risk individuals—even those with low cholesterol—who are otherwise invisible to standard screening algorithms.
It is an unfortunate reality that markers are frequently ignored because there is no FDA-approved drug to address it, which is a therapeutic blindspot. The conventional model demands a drug to justify a test, but applying physiological logic, systemic inflammation is a structural reality that can be profoundly modulated by non-pharmaceutical protocols. Naturopathic Medicine provides an arsenal of safe, natural options that effectively lowers low-grade inflammation. HSCRP serves as a critical prognostic indicator, and utilizing benign natural compounds to suppress this physiological threat is a highly pragmatic, low risk strategy.
Summary:
Clinical Bottom Line
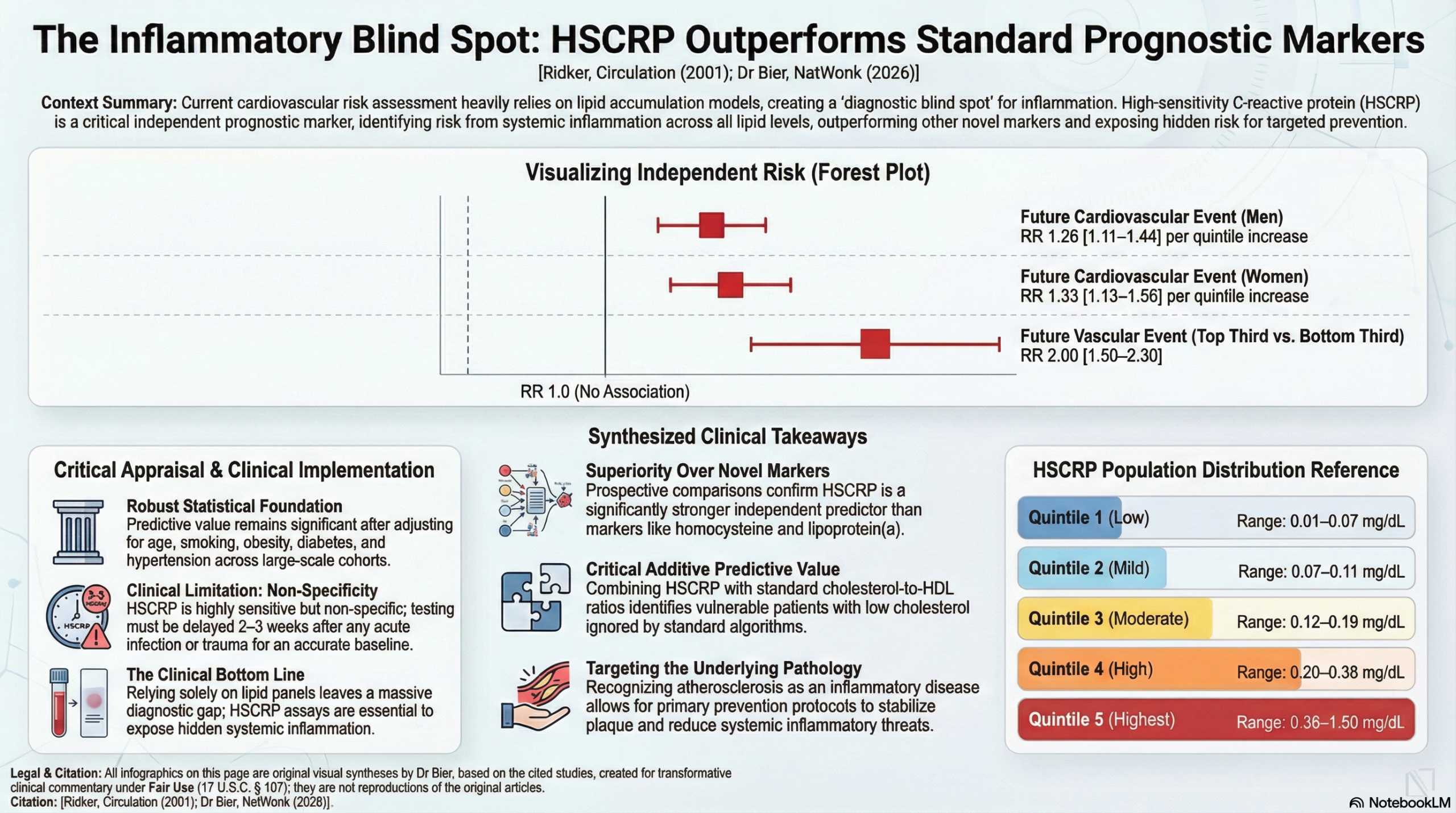
This landmark perspective and review of prospective data establish high-sensitivity C-reactive protein (HSCRP) as a powerful, independent predictor of cardiovascular risk in apparently healthy individuals. While traditional lipid screening remains the standard, adding HSCRP testing significantly improves the accuracy of global risk prediction—even in patients with low cholesterol levels. Clinicians should view HSCRP not as a replacement for LDL monitoring, but as a “tie-breaker” or additive tool to identify high-risk individuals who might otherwise be missed by standard algorithms. However, its clinical utility is contingent on using “high-sensitivity” assays rather than standard CRP tests, and results must be interpreted cautiously in the presence of acute infection or chronic inflammatory conditions.
Results in Context
- Main Results: HSCRP is a strong independent predictor of future myocardial infarction, stroke, and peripheral arterial disease. In a cohort of 22,000 men, those in the highest quartile of HSCRP had a 3-fold increase in the risk of myocardial infarction.
- Definitions & Context: The paper focuses on prognostic value—the ability of a marker to predict the likely course of a disease. HSCRP measures low-grade systemic inflammation, which plays a major role in the instability and rupture of atherosclerotic plaques.
- Additive Predictive Value: When HSCRP is added to the total cholesterol:HDL ratio, the predictive power is significantly higher than using lipids alone (P<0.001). HSCRP has additive value at all lipid levels, including those considered “low risk”.
- Comparison to Other Markers: In direct comparisons, HSCRP was a stronger predictor of risk than other “novel” markers like homocysteine or lipoprotein(a).
- Biomarker Technology: The study emphasizes High-Sensitivity CRP (HSCRP), which uses automated immunoassays capable of detecting CRP levels in the “low-normal” range (below 0.3~mg/dL), whereas standard CRP assays are only designed to detect gross inflammation (above 0.5 to 1.0~mg/dL).
Assertive Critical Appraisal
- Appraisal of Biomarker Claim (Prognostic vs. Predictive): * The authors primarily establish HSCRP as a prognostic marker for primary prevention in healthy populations.
- A predictive claim is also suggested: the paper notes that the benefit of aspirin and statins appears greater in patients with elevated HSCRP. However, the authors appropriately caution that while the possibility of using HSCRP to target statin therapy is “promising,” it requires further direct prospective testing to confirm if “number needed to treat” is actually reduced.
- Reporting Quality Assessment (REMARK): * The paper clearly specifies the target population (apparently healthy men and women) and the assay methodology (automated high-sensitivity systems).
- It provides a clear quintile-based system for determining “cut-points”: Low (<0.07 mg/dL), Mild (0.07–0.11), Moderate (0.12–0.19), High (0.20–0.38), and Highest (>0.38).
- Critical Omission: The authors acknowledge that the utility of HSCRP across different ethnic groups remains uncertain, which is a significant limitation for a global risk marker.
- Confounding Factors: A major strength is that the predictive value of HSCRP remained significant even after adjusting for age, smoking, obesity, diabetes, and hypertension.
- Clinical Limitations: The non-specific nature of HSCRP is its “Achilles’ heel.” Because it increases with any trauma or infection, testing must be avoided for 2–3 weeks following an acute illness to prevent misclassification.
Applicability
HSCRP testing is highly applicable in general practice because the assays are inexpensive, standardized, and commercially available. It is particularly relevant for patients who fall into “intermediate risk” categories where the decision to start long-term preventive therapy (like statins) is unclear.
Research Objective
To evaluate the evidence supporting HSCRP as an independent predictor of cardiovascular risk and to assess its potential as an adjunct for global risk assessment in primary prevention.
Study Design
This is a narrative review and synthesis of data from multiple large-scale prospective epidemiological studies (including the Women’s Health Study, Physicians’ Health Study, and MONICA Augsberg cohort).
Setting and Participants
The analysis draws on data from over 5,000 Americans to establish population distributions and several cohorts totaling tens of thousands of “apparently healthy” men and women without known cardiovascular disease.
Bibliographic Data
- Title: High-Sensitivity C-Reactive Protein: Potential Adjunct for Global Risk Assessment in the Primary Prevention of Cardiovascular Disease
- Author: Paul M. Ridker
- Journal: Circulation
- Year: 2001
- DOI: 10.1161/01.CIR.103.13.1813
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.