
Comment:
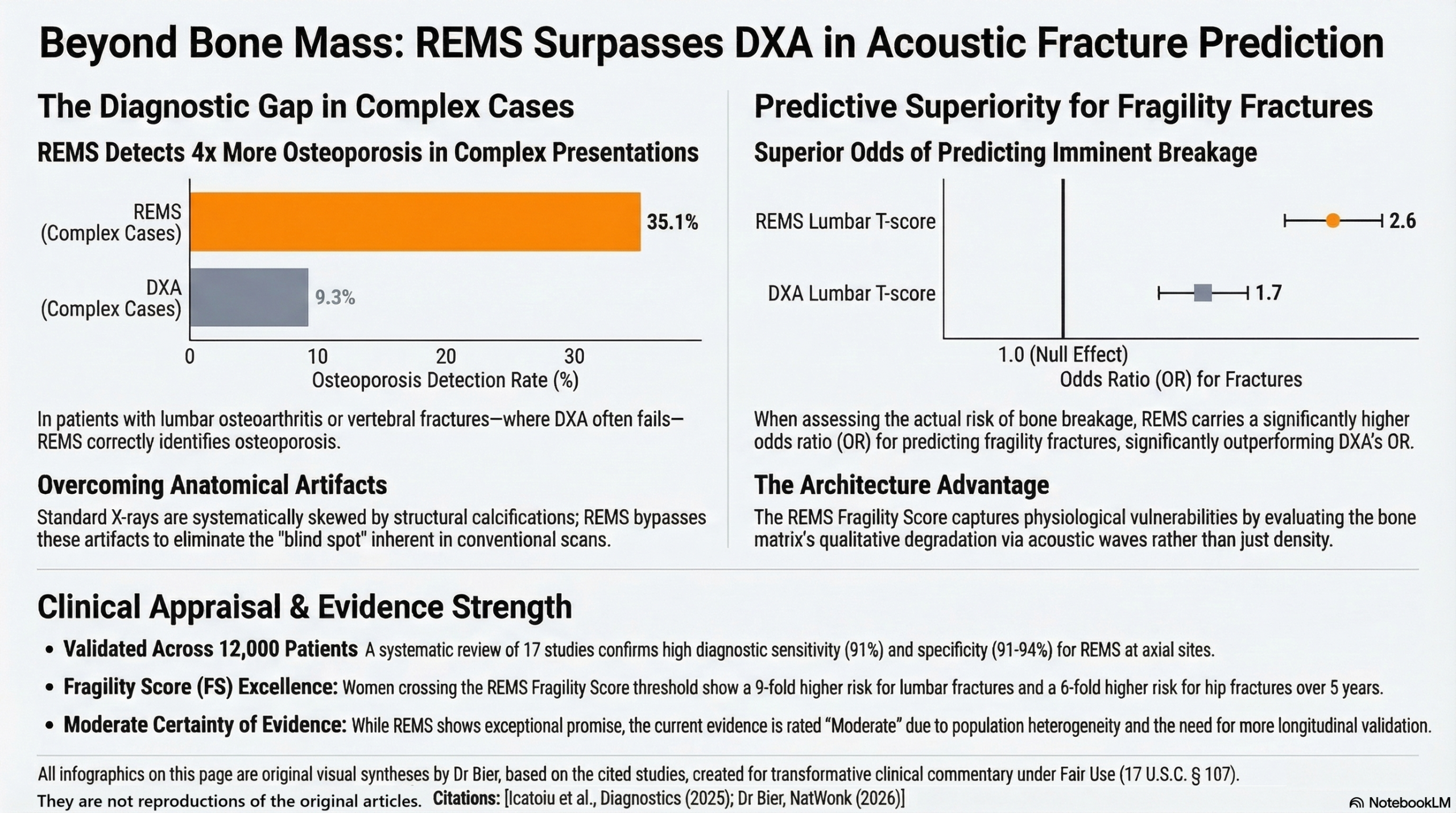
With all testing of secondary markers it’s always important to remember that there’s never a straight line correlation. I don’t care about cholesterol – I care about cardiovascular events. And similarly a patient does not suffer from a low T-score; they suffer from a fracture. Evaluating fracture risk within this systematic review there is the disconnect between the trust placed in DXA and its demonstrable inferiority when identifying imminent bone fracture. The data in this review reveals that REMS is a far superior predictor of actual fragility fractures, carrying an Odds Ratio of 2.6 compared to DXA’s 1.7.
Fracture risk is a function of both bone mass and architecture. Relying exclusively on the X-ray attenuation of DXA misses the qualitative reality of the bone’s internal scaffolding. REMS captures this missing variable through its acoustic Fragility Score (FS), assessing the qualitative degradation of the bone matrix independently of its mass. The longitudinal data validates this physiological advantage: in a 5-year prospective cohort, women who crossed the threshold of the REMS Fragility Score were 9 times more likely to suffer an actual lumbar fracture—and 6 times more likely to suffer a hip fracture—than those with normal acoustic scores, which vastly outperforming the predictive utility of relying on a standard DXA bone mass measurement.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This systematic review suggests that Radiofrequency Echographic Multi Spectrometry (REMS) is a reliable, radiation-free alternative to Dual-energy X-ray Absorptiometry (DXA) for diagnosing osteoporosis and assessing fracture risk. The evidence indicates strong diagnostic agreement with DXA (63.6–90%) and potentially superior performance in patients with anatomical artifacts (e.g., osteoarthritis or calcifications) that often lead to DXA overestimating bone mineral density (BMD). While the Fragility Score (FS) shows promise as an independent predictor of incident fractures, the long-term utility of REMS requires further validation through extensive prospective longitudinal studies.
Results
- Summary of Results: The reviewed studies demonstrated high diagnostic concordance between REMS and DXA, generally ranging from 82.2% to 88.8%. Correlation coefficients for BMD typically exceeded 0.90 for both the lumbar spine and femoral neck in general populations.
- Sensitivity and Specificity: REMS showed a sensitivity of approximately 91% and specificity of 91-94% for detecting osteoporosis at axial sites.
- Performance in Complex Cases: REMS identified osteoporosis in 35.1% of cases where DXA identified only 9.3%, specifically in patients with lumbar osteoarthritis or vertebral fractures.
- Fragility Score (FS): In a 5-year prospective study, the FS demonstrated a 9-fold higher risk for fragility fractures in the lumbar spine compared to standard BMD T-scores, with an Area Under the Curve (AUC) of 0.78–0.81.
Assertive Critical Appraisal
- Certainty of Evidence (GRADE Framework): The overall certainty of evidence is Moderate. While diagnostic accuracy and repeatability are well-documented, most included studies were cross-sectional. The recommendations for using REMS in frail or specific populations were rated “strongly in favor,” but its ability to predict incident fractures and provide short-term monitoring was rated “weakly in favor” by experts due to limited longitudinal data.
- Heterogeneity: The review acknowledges substantial heterogeneity in study populations, which included primary/secondary osteoporosis, chronic kidney disease, and anorexia nervosa. In these special cohorts, correlations between REMS and DXA were often weaker (e.g., $r=0.35$ to $0.65$), likely due to inherent inaccuracies in the DXA “gold standard” when artifacts are present.
- Publication Bias: The authors noted that the search was limited to three databases and English-language literature, potentially introducing publication bias by excluding non-English studies or grey literature.
- Risk of Bias in Included Studies: Using the CASP checklist, most cross-sectional studies were found to have well-defined cohorts and rigorous designs. However, several were limited by small sample sizes or the exclusion of severely obese patients ($BMI > 40~kg/m^2$), for whom REMS is not yet validated.
- Reporting Quality Assessment (PRISMA): The systematic review followed PRISMA guidelines and was registered in PROSPERO. It included a clear flow diagram and detailed inclusion/exclusion criteria, though the omission of the search term “DEXA” may have limited the number of retrieved articles despite “DXA” being the preferred scientific term.
Research Objective
The review aimed to evaluate the accuracy of REMS technology in diagnosing osteoporosis and predicting fragility fracture risk compared to the current gold standard, DXA.
Study Design
This was a systematic review of English-language literature published between January 2015 and December 2024. The synthesis included data from 17 original articles (2 prospective cohorts and 15 cross-sectional studies).
Setting and Participants
The review encompassed a total of 11,664 patients (79.85% female) aged 30 to 90 years across Europe, Asia, and the Americas. Participant groups included postmenopausal women, men, and patients with conditions affecting bone metabolism (e.g., T2DM, CKD, and Osteogenesis Imperfecta).
Bibliographic Data
- Title: Radiofrequency Echographic Multi Spectrometry-A Novel Tool in the Diagnosis of Osteoporosis and Prediction of Fragility Fractures: A Systematic Review
- Authors: Icatoiu E, Vladulescu-Trandafir A-I, Groseanu L-M, et al.
- Journal: Diagnostics
- Year: 2025
- DOI: 10.3390/diagnostics15050555
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.