
Comment:
Although meta-analyses are considered to be a higher level method, there are significant issues with them. I am always suspicious of pooled averages that ignore massive internal contradictions. This study reports high I2 for all-cause dementia ranging from 81.5% to 93%, which is a red flag. This number indicates that the studies being combined are so wildly different in their methods and results that averaging them together is clinically meaningless. When you add the confirmed publication bias (Egger’s p = 0.0105), it becomes clear we are looking at a sanitized version of the truth.
A high I2 means the studies were “messy” and disagreed with each other a vast majority of the time. Additionally, “publication bias” suggests that researchers likely buried the studies that showed statins didn’t work or caused harm, only publishing the “successful” ones. When you take a pile of mismatched studies and ignore the “failed” ones, you aren’t doing science; you’re doing marketing.
Additionally, and even more importantly, although the top line results show a “protective” signal from statin use, the RCTs like PROSPER and HOPE-3 consistently show no cognitive benefit. This discrepancy is likely explained by Healthy User Bias. In these 55 observational studies, the people taking statins aren’t just taking a pill; they are often the same people who follow medical advice, exercise more, and eat better. Healthy User Bias is a hidden variable that ruins data. If people who take statins are generally more health-conscious than those who don’t, they are naturally at a lower risk for dementia because of their lifestyle, not the drug. The statin is essentially a “badge” for someone who takes care of themselves. When researchers see these people doing well, they mistakenly credit the pill for the neuroprotection that actually came from the patient’s own healthy habits. It’s why observational studies will frequently show benefits that disappear in RCTs.
The Structural Collision: Observational Volume vs. RCT Failure
-
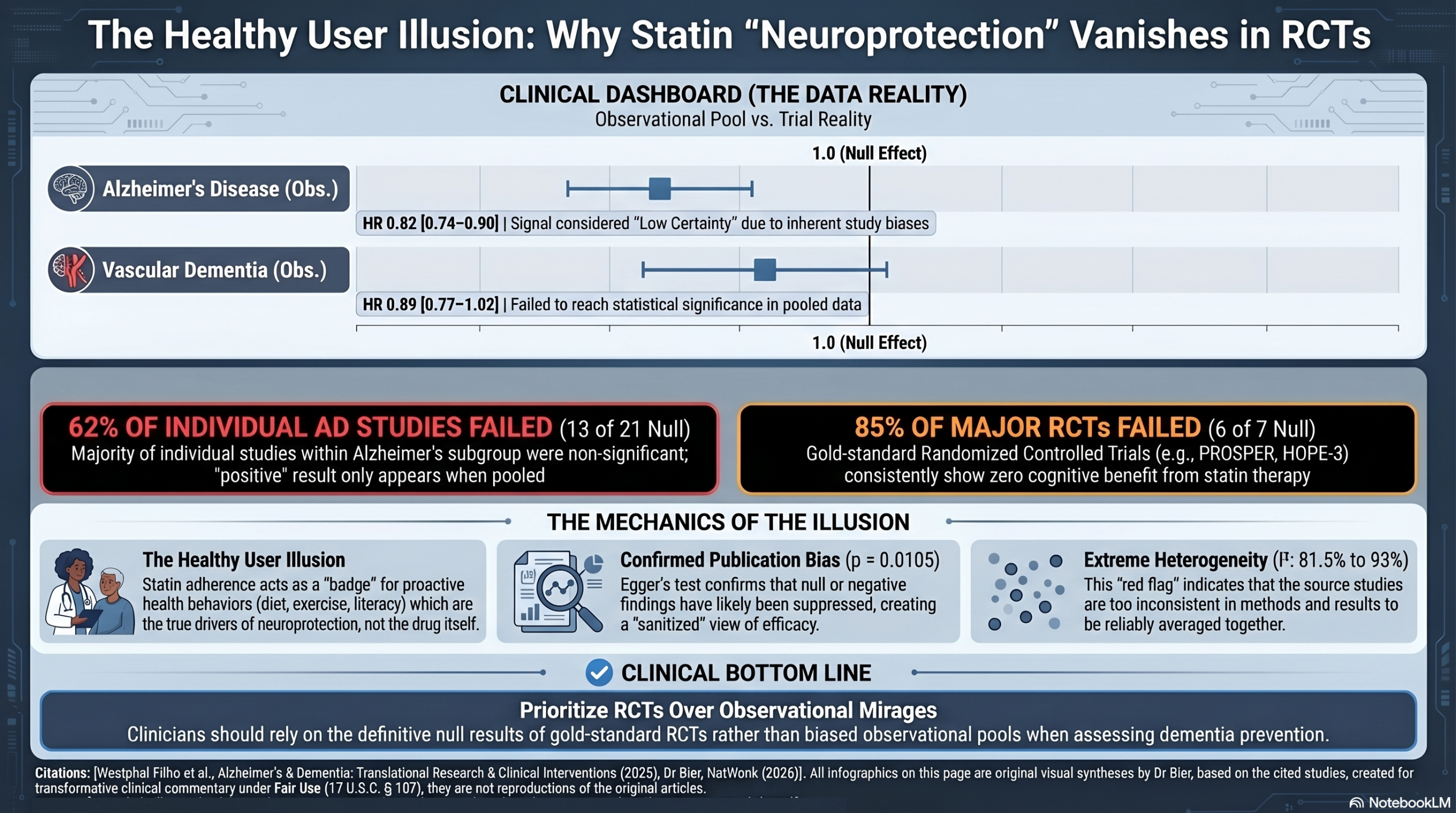
The RCT Scorecard: A critical audit of the Randomized Controlled Trials (RCTs) cited in the Discussion reveals a near-total failure of the drug to move the needle under controlled conditions. Of the major trials examined—including PROSPER, HOPE-3, the Simvastatin Heart Protection Study, and the Feldman and Sano established dementia trials—6 out of 7 (85%) failed to demonstrate a significant primary cognitive benefit.
-
Observational Masking: While the meta-analysis leverages a massive volume of 7 million observational patients to force a “significant” pooled p-value, this volume masks a high internal failure rate among the source studies. As confirmed by the Forest plot Figure 4A, 62% (13 out of 21) of the Alzheimer’s Disease subgroup studies were individually non-significant.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
This meta-analysis suggests that statin use is associated with a reduced risk of all-cause dementia and Alzheimer’s disease (AD); however, the certainty of this evidence is rated as Low. While the pooled results are statistically significant, the analysis relies entirely on observational data subject to “healthy user bias,” demonstrates massive statistical heterogeneity, and suffers from confirmed publication bias. Furthermore, the significant pooled effect is heavily reliant on combining numerous individual studies that failed to show a significant benefit on their own.
Results
Summary of Results: * All-Cause Dementia: Statin use was associated with a significant reduction in the risk of all-cause dementia compared to nonusers (Hazard Ratio [HR] 0.86; 95% CI: 0.82 to 0.91).
- Alzheimer’s Disease (AD): Statin use was associated with a reduced risk of AD (HR 0.82; 95% CI: 0.74 to 0.90).
- Vascular Dementia (VaD): The association between statin use and VaD risk was not statistically significant in the primary HR analysis (HR 0.89; 95% CI: 0.77 to 1.02). (Note: A Hazard Ratio of 0.86 means there was a 14% reduction in the hazard, or rate, of developing dementia in the statin group compared to the control group over the study periods).
Assertive Critical Appraisal
Certainty of Evidence (GRADE Framework): The overall certainty of the evidence is Low. The evidence is downgraded because it relies exclusively on observational study designs rather than randomized controlled trials, exhibits exceptionally high inconsistency (heterogeneity) across study results, and shows clear evidence of publication bias.
Heterogeneity: The reported heterogeneity statistic for the primary all-cause dementia outcome is an I2 of 81.5% to 93%. The I2 statistic represents the percentage of variation across studies due to real differences rather than just chance. An I2 this high indicates substantial heterogeneity, suggesting the studies are showing widely different results (likely due to varied diagnostic methods, statin types, and exposure durations) and that the pooled average should be interpreted with extreme caution.
Publication Bias: The authors assessed for publication bias using both a funnel plot and the Egger’s test. The Egger test results revealed the presence of significant publication bias for the all-cause dementia outcome (p=0.0105). Publication bias is a common threat that can lead to an overestimation of treatment effects, as it suggests studies reporting null or negative results are missing from the published literature.
Risk of Bias in Included Studies: The authors assessed the risk of bias using the Newcastle-Ottawa Scale (NOS). They reported a moderate to low risk of bias among the included studies, with an average score of 7.62 out of 9. However, because all 55 studies were observational, they remain highly susceptible to “healthy user bias,” meaning patients who take statins may also engage in other health-promoting behaviors that reduce dementia risk.
Special Consideration for Pooled Results: . In the AD hazard ratio forest plot (Figure 4A), 13 out of the 21 individual study subgroups cross the null line (1.0), meaning they are not individually significant . Similarly, in the primary all-cause dementia forest plot (Figure 2), roughly half of the study subgroups in the general pool failed to achieve individual statistical significance .
- It is important to note that while the overall pooled result is statistically significant, this conclusion is derived from a collection of smaller studies, the majority of which did not find a significant effect on their own.
- This scenario often occurs when individual studies are underpowered (too small) to detect a modest but real treatment effect. By combining their data, the meta-analysis increases the overall statistical power, which can reveal a consistent trend that was not apparent in the smaller studies.
- However, this finding should be interpreted with caution. It is crucial to assess for significant heterogeneity (differences between studies) and the potential for publication bias (the possibility that unpublished negative studies are missing), as either of these factors could lead to a misleading pooled result. In this paper, both massive heterogeneity and confirmed publication bias are present.
Reporting Quality Assessment (PRISMA): The review generally adheres well to PRISMA reporting standards. The authors included a PRISMA flow diagram detailing the study selection process (Figure 1) , and they adequately described their search strategy across PubMed, Cochrane, and Embase, including the syntax used.
Research Objective
The objective was to evaluate the association between statin use (Intervention) and the incidence of all-cause dementia, Alzheimer’s disease, and vascular dementia (Outcomes) in patients aged 18 years or older (Population) compared to nonusers (Control).
Study Design
This is a systematic review and meta-analysis of observational studies, specifically encompassing both cohort and case-control study designs. The researchers utilized random-effects models for their meta-analyses to account for expected high heterogeneity.
Setting and Participants
The review included 55 observational studies comprising a total of 7,786,651 participants. The studies were geographically distributed across the Americas, Asia, Europe, and Oceania.
Bibliographic Data
- Title: Statin use and dementia risk: A systematic review and updated meta-analysis
- Authors: Fernando Luiz Westphal Filho, Artur Menegaz de Almeida, Fernanda Moraes Tamashiro, et al.
- Journal: Alzheimer’s & Dementia: Translational Research & Clinical Interventions
- Year: 2025
- DOI: 10.1002/trc2.70039
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.