
Comment:
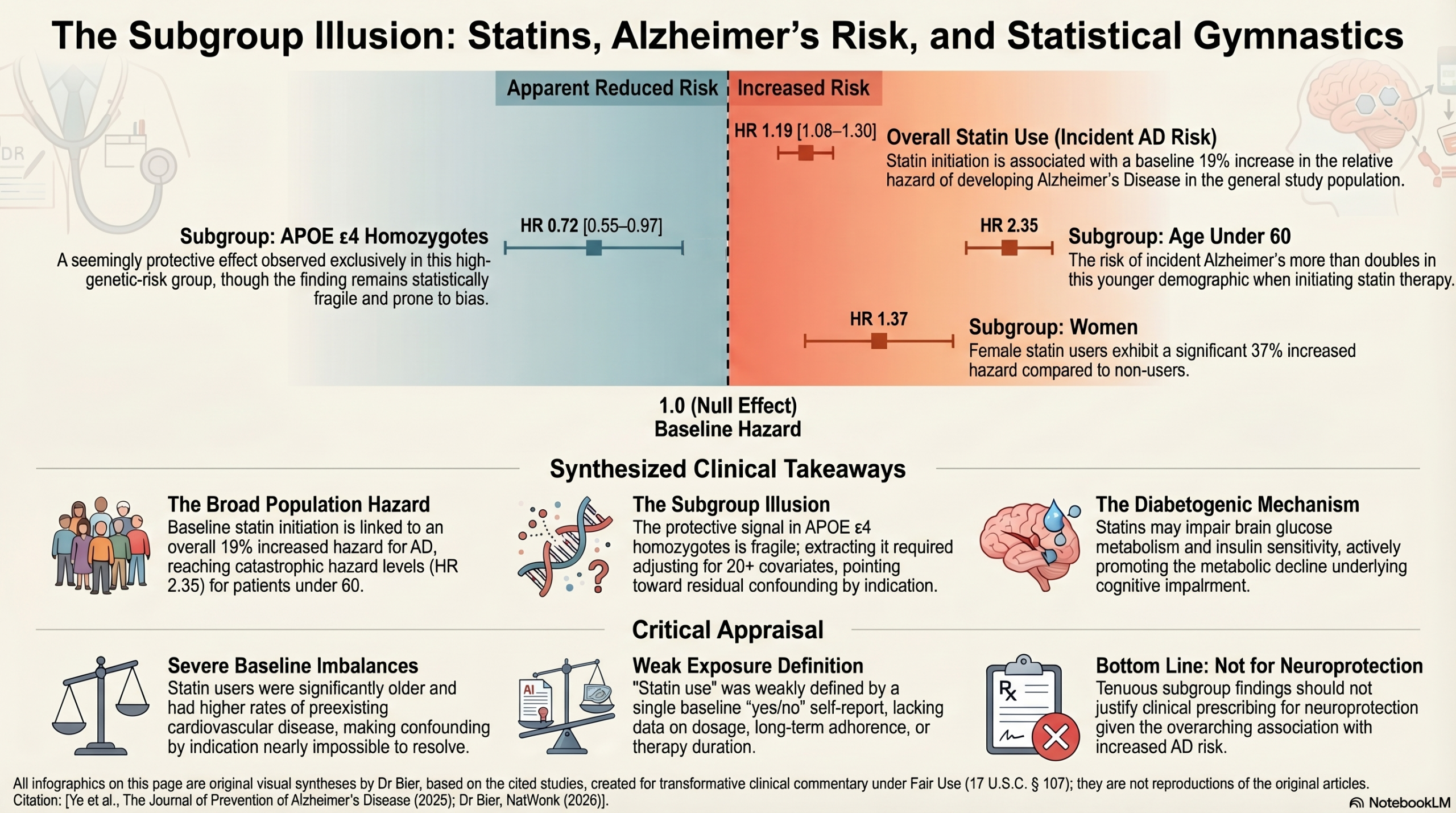
This UK Biobank cohort study highlights a conflict between the narrative of statins as a vascular panacea and the documented reality that their use is associated with a 19% increased risk of incident Alzheimer’s disease (HR = 1.19).
Looking carefully at the “protective” finding in APOE ε 4 homozygotes (HR = 0.72), there are a lot of reasons to be skeptical. This subgroup signal required adjusting for more than 20 covariates across three models—a level of statistical gymnastics that suggests residual confounding rather than true efficacy. Furthermore, while the general population faces an elevated risk, the signal for those under 60 is catastrophic (HR = 2.35). We should be cautious of over-interpreting a fragile subgroup finding (95% CI: 0.55–0.97) when the broader data indicates a significant risk for the majority.
The Physiological Filter
The biological logic here is grounding: the neurotoxic signal is likely driven by the diabetogenic effect of statins. By impairing insulin sensitivity and brain glucose metabolism, these drugs may be inducing the very metabolic decline they are purported to prevent. The data confirms that there was never a cognitive benefit to begin with; rather, the apparent mental detriment seen in users is merely a statistical artifact of their sicker baseline status. Once these comorbidities are properly adjusted for, the medication’s impact on global cognitive performance is revealed to be entirely neutral (β = 0.00).
Although it’s pitched as neuroprotective, for the vast majority of patients—especially women (HR = 1.37) and those under 60—statin initiation represents a significant hazard.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This cohort study demonstrates an overall association between baseline statin use and an increased risk of incident Alzheimer’s disease, though it suggests a potentially protective effect in the subgroup of patients carrying two APOE ε4 alleles. However, it is critical to recognize that this is an observational study heavily reliant on complex statistical adjustments to control for significant baseline imbalances; therefore, it is not possible to conclude that statin use directly influences disease risk, and the reliability of the APOE ε4 subgroup protection is highly tenuous.
Results in Context
- Main Results:
- In the fully adjusted model (Model 3), statin use was associated with a 19% increased risk of developing Alzheimer’s Disease (AD) compared with nonuse (Hazard Ratio [HR] 1.19, 95% CI 1.08 to 1.30).
- However, when stratified by genetic risk, patients carrying two APOE ε4 alleles who used statins demonstrated a lower risk of AD compared to nonusers (HR 0.72, 95% CI 0.55 to 0.97).
- Statins also appeared protective in older adults (≥60 years) and those with baseline cardiovascular diseases like stroke or heart failure.
- Definitions: A Hazard Ratio (HR) of 1.19 means that the statin group had a 19% higher relative hazard of being diagnosed with AD over the study period compared to the non-statin group.
- Participants: The final analysis included 371,019 eligible participants. There were 315,834 nonusers and 55,185 statin users at baseline. Over the follow-up, 2,951 participants developed AD.
Assertive Critical Appraisal
Limitations & Bias (Robustness of the APOE ε4 Finding)
A critical examination of the “protective” finding in APOE ε4 carriers reveals significant fragility.
- Statistical Gymnastics and Residual Confounding: Uncovering this interaction required the authors to adjust for more than 20 covariates across three models—including demographics, lifestyle variables, inflammatory markers, and a vast array of extensive comorbidities. When an observational study requires this degree of heavy multi-variable adjustment to tease out a subgroup effect, the risk of unmeasured, residual confounding remains exceptionally high.
- Baseline Imbalances: Statin users in this cohort had fundamentally different baseline risk profiles; they were older, had a higher prevalence of cardiovascular disease, and exhibited a higher raw incidence of AD before adjustment (1.65% vs 0.65%). Controlling for this degree of confounding by indication is incredibly difficult in retrospective data.
- Weak Exposure Definition: The study defined “statin use” merely as a “yes/no” based on self-reported questionnaires or interviews at a single baseline timepoint. The investigators had no data on medication dosage, long-term adherence, or duration of therapy over the 9-year follow-up period.
- Borderline Precision: The confidence interval for the benefit in the two-allele group (95% CI 0.55 to 0.97) is wide and approaches the null value of 1.0.
Because of these factors, the finding of protection in APOE ε4 carriers is highly susceptible to artifact and bias. It should be viewed strictly as hypothesis-generating and should not guide clinical prescribing practices.
Reporting Quality Assessment (STROBE) The authors adequately describe their methods for attempting to control for potential sources of confounding by utilizing sequential multivariate adjustment models and performing robust sensitivity analyses, such as accounting for competing risks and concurrent aspirin use. However, they rightfully acknowledge that despite these adjustments, unmeasured biases remain a core limitation of their methodology.
Applicability The study population was entirely restricted to volunteers of White European ancestry. Coupled with the well-known “healthy volunteer” selection bias inherent to the UK Biobank cohort, these findings may not safely generalize to more diverse, real-world clinical populations.
Research Objective The objective was to examine the association of statins use with the risk of cognitive impairment and incident AD, and to assess the moderating roles of genetic susceptibility and other individual-related factors.
Study Design A longitudinal, population-based prospective cohort study.
Setting and Participants Participants were drawn from the UK Biobank, recruited between 2006 and 2010 across 22 assessment centers in England, Scotland, and Wales. The study included individuals aged 40 and older who were free of dementia, prevalent neurological or psychiatric disorders, and cancer at baseline.
Bibliographic Data
- Title: Association of statins use and genetic susceptibility with incidence of Alzheimer’s disease
- Authors: Zirong Ye, Jiahe Deng, Xiuxia Wu, Jingwen Cai, Sicheng Li, Xiaochun Chen, Jiawei Xin
- Journal: The Journal of Prevention of Alzheimer’s Disease
- Year: 2025
- DOI: https://doi.org/10.1016/j.tjpad.2024.100025
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.