
Comment:
This is another in a long line of studies where a randomized trial fails to show the benefit seen in observational cohorts. It is crucial to prioritize hard, randomized data because it is the only way to strip away the Healthy User Bias that plagues nutritional and pharmaceutical research. In observational studies, people who take statins are often the same “healthier users” who exercise more and follow medical advice, which creates a deceptive protective signal for the brain. However, when we apply the physiological filter of a double-blind RCT like in this study, that bias is neutralized through randomization. While observational studies often credit statins for the lifestyle-driven outcomes of health-conscious patients, this RCT provides a clear answer. After 5.7 years of treatment in participants ≥ 70 years old, there was a mean decline in cognitive scores across the board, with no benefit from rosuvastatin, blood pressure lowering, or their combination. This confirms that the supposed “neuroprotective” effect seen in less rigorous models is a statistical ghost. The improvements seen in observational trials are not real, but a function of baseline differences between users and non-users.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
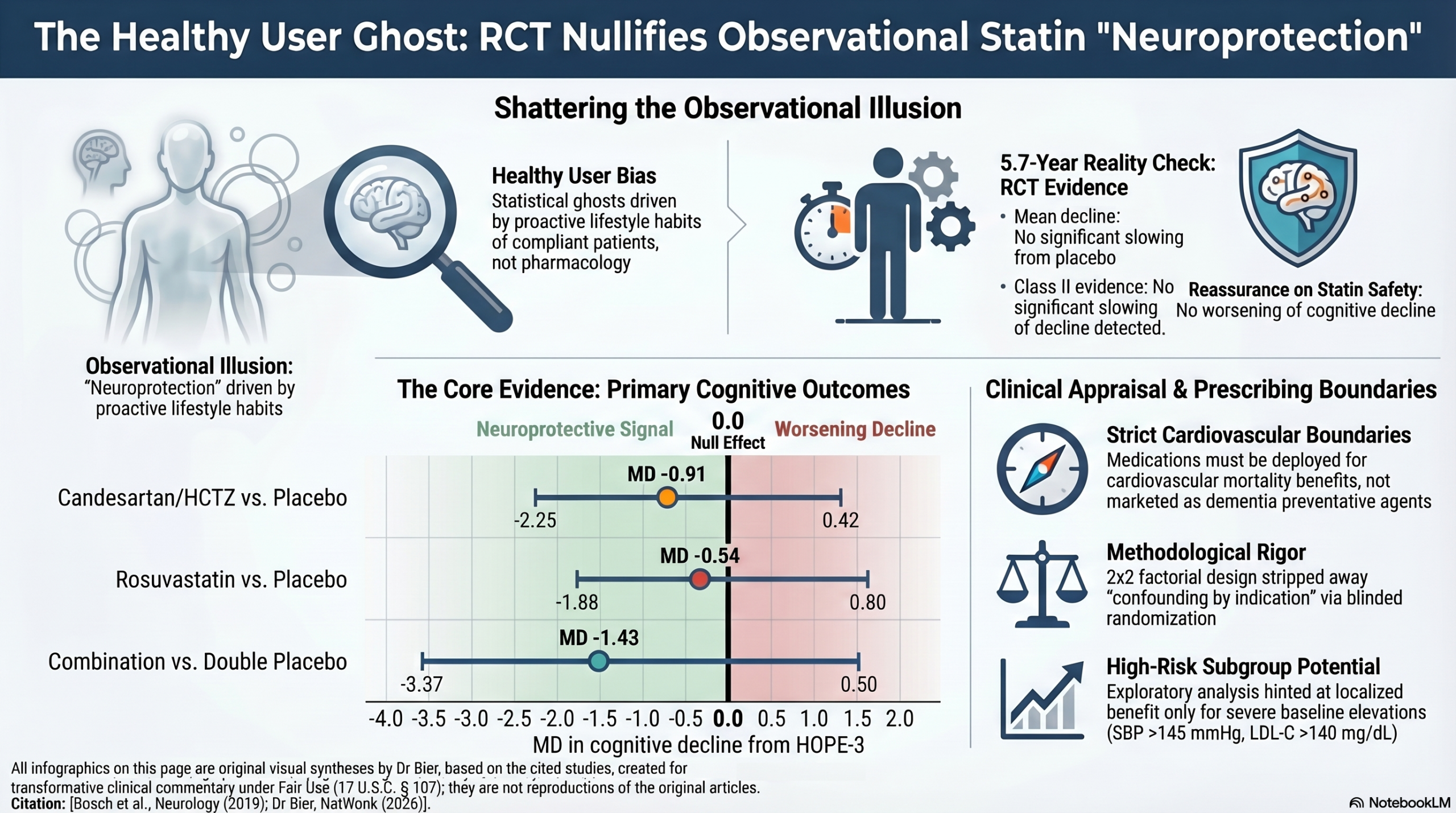
This study provides Class II evidence that long-term treatment with a combination of blood pressure (BP) lowering (candesartan/hydrochlorothiazide) and cholesterol lowering (rosuvastatin) does not significantly slow cognitive decline in older adults at intermediate cardiovascular risk. While there was a mean decline in cognitive scores across all groups over the 5.7-year follow-up, no significant differences were observed between active treatments and placebo for the primary cognitive measure. However, an exploratory subgroup analysis suggests a potential benefit for combined therapy in individuals with the highest baseline levels of both systolic BP and LDL cholesterol. For the general older population at intermediate risk, these medications should be prescribed for their proven cardiovascular benefits rather than for the prevention of cognitive decline.
Results in Context
Primary Outcome: The primary outcome was the change in the Digit Symbol Substitution Test (DSST) score from baseline to study end. The DSST evaluates psychomotor speed, attention, and executive function; a decrease of \ge 5 points is considered a meaningful decline.
- Candesartan/HCTZ vs. Placebo: Mean difference -0.91 (95% CI -2.25 to 0.42), p=0.29.
- Rosuvastatin vs. Placebo: Mean difference -0.54 (95% CI -1.88 to 0.80), p=0.91.
- Combination vs. Double Placebo: Mean difference -1.43 (95% CI -3.37 to 0.50), p=0.50.
- None of these results reached statistical significance, indicating no treatment effect on the rate of cognitive decline.
Key Secondary & Specialized Outcomes:
- Secondary Cognitive Measures: No significant differences were found in the modified Montreal Cognitive Assessment (mMoCA) or Trail Making Test Part B (TMT-B) across any treatment arms.
- Functional Outcomes: Approximately 20% of participants developed new impairments in basic activities of daily living (ADL), but this did not vary by treatment group.
- Dementia and Institutionalization: Only 16 individuals developed dementia and 4 were institutionalized, with no significant differences between groups.
Harms and Adverse Events: The trial specifically addressed concerns regarding statins and cognition. The results showed that rosuvastatin did not worsen cognitive decline compared to placebo, providing reassurance against observational data suggesting statins might impair memory.
Assertive Critical Appraisal
Risk of Bias (RoB 2 Framework): Overall Judgment: Low Risk. The study was a well-executed, double-blind, randomized, placebo-controlled trial. Randomization and allocation concealment were robustly managed through a blinded central system.
Subgroup Analyses: The authors highlight a significant finding in a post-hoc exploratory subgroup (n=181) of participants with the highest baseline SBP (>145 mm Hg) and LDL-C (>140 mg/dL), where combination therapy reduced cognitive decline (p=0.04 for interaction). Critique: While biologically plausible—as those with the most to gain from risk factor modification often show the greatest benefit—this result should be viewed with skepticism. Small subgroup sizes and multiple testing increase the risk of a type I error (false positive).
Reporting Quality Assessment (CONSORT): The reporting quality is high. The authors included a CONSORT participant flow diagram (Figure 1), clearly showing that of the 3,086 eligible participants \ge 70 years old, 2,361 completed baseline assessments and 1,626 completed the full study follow-up.
Missing Data Appraisal: A significant limitation is that only 76% of surviving participants completed the final DSST. The authors addressed this using two different imputation techniques (matching and multiple imputation). Sensitivity analyses using these methods yielded results consistent with the primary analysis, which increases confidence that the missing data did not significantly bias the outcome.
Applicability: The population consisted of older adults (mean age 74) at intermediate cardiovascular risk without prior CVD. This is highly relevant to general primary care. However, the participants may have been “healthier than average” due to selection bias (27% of those eligible refused to participate), which might limit generalizability to more frail elderly populations.
Research Objective
To determine if long-term treatment with candesartan/hydrochlorothiazide, rosuvastatin, or their combination can slow cognitive decline in older adults at intermediate cardiovascular risk.
Study Design
A double-blind, randomized, placebo-controlled clinical trial using a 2 times 2 factorial design.
- Total Participants: 2,361 completed baseline; 1,626 completed end-of-study assessments.
- Median Follow-up: 5.7 years.
Setting and Participants
- Setting: 228 centers across 21 countries.
- Participants: Men ≥ 55 and women ≥ 60/65 with cardiovascular risk factors; the cognition substudy was restricted to those ≥ 70 years old.
- Exclusion: Known cardiovascular disease or a clear clinical indication for the study drugs.
Bibliographic Data
- Title: Effects of blood pressure and lipid lowering on cognition: Results from the HOPE-3 study
- Authors: Jackie Bosch, Martin O’Donnell, Balakumar Swaminathan, et al.
- Journal: Neurology
- Year: 2019
- DOI: 10.1212/WNL.0000000000007174
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.