
Comment:
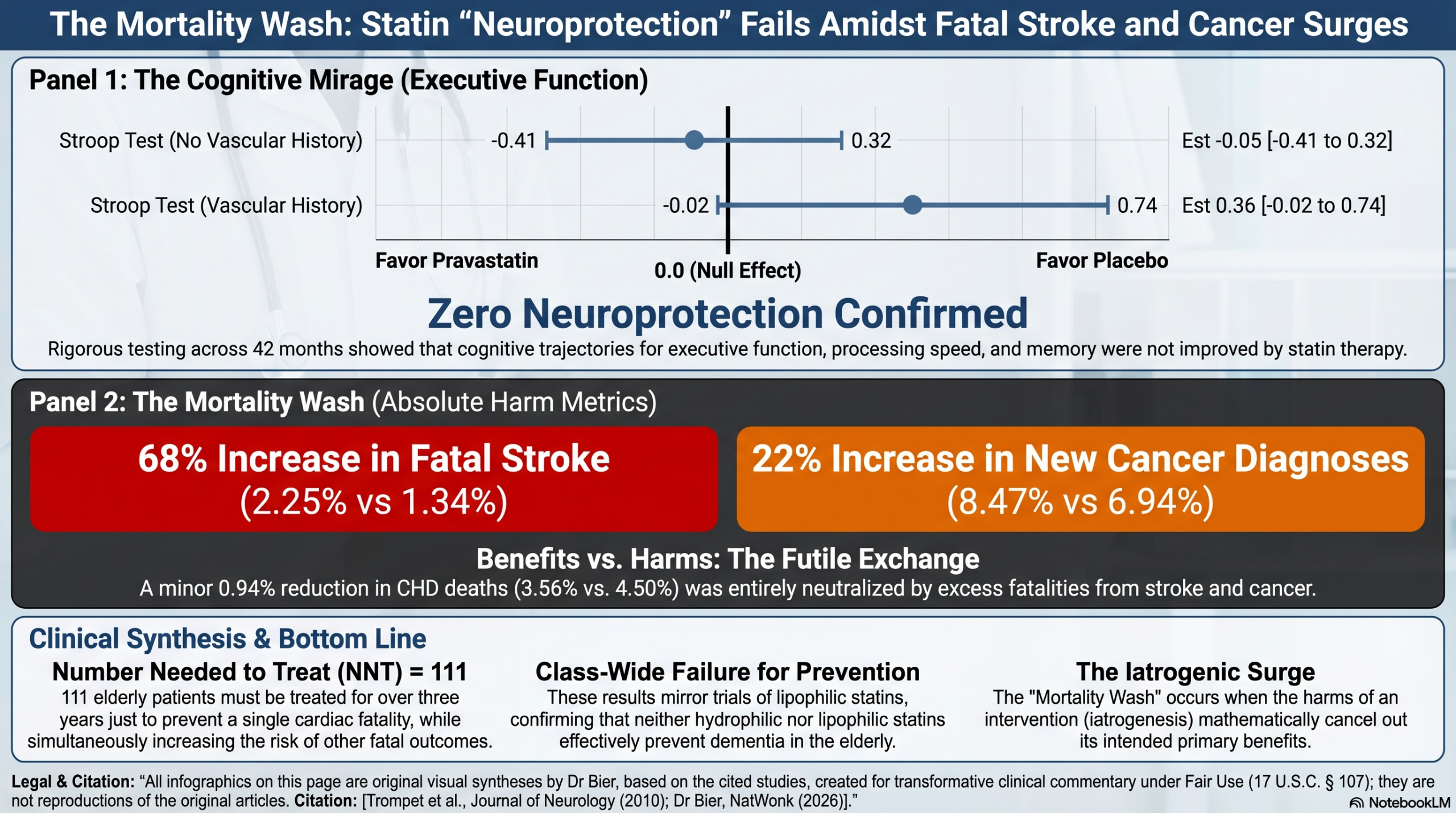
The findings in this randomized controlled trial of 5,804 elderly participants are unequivocal: after a mean follow-up of 42 months, pravastatin demonstrated absolutely no difference in cognitive decline across any domain—including executive function, processing speed, or memory.
It also celebrates a 24% RRR in cardiovascular mortality while the Absolute Risk Reduction (ARR) was a mere 0.9%. This translates to a requirement to treat 111 elderly patients for over three years to prevent a single cardiovascular death. And yet there is not improvement in overall survival, which means the treatment itself is causing other deaths.
And where are those extra deaths coming from – a statistically significant 22% increase in new cancer diagnoses (p = 0.02) and a 68% increase in fatal strokes (p = 0.015). in the treatment arm. This creates a “mortality wash” where the lives saved from coronary heart disease were effectively neutralized by additional deaths from cancer and stroke. And that doesn’t take into account the extra 1.19% increase in non-fatal cancer diagnoses,
This is not the first time we have seen an increase in cancer with statin treatments, however that is often dismissed as an observational finding – cancer patients are not able to make cholesterol versus low cholesterol increases cancer risk. Because this is a randomized trial, that deflection is disproven – the increase in cancer seen with statin use can not be due to reverse causation.
| Outcome | Pravastatin | Placebo | p-value | Clinical Signal |
| Cardiovascular Death | 3.3% | 4.2% | 0.043 | 0.9% Absolute Benefit |
| Fatal Stroke | 2.25% | 1.34% | 0.015 | 0.91% Absolute Harm |
| Cancer Death | 3.94% | 3.60% | 0.55 | 0.34% Increase (Non-Sig) |
| New Cancer Diagnosis | 8.47% | 6.94% | 0.02 | 1.53% Absolute Harm |
| All-Cause Mortality | 15.60% | 15.31% | 0.89 | The Mortality Wash |
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This high-quality randomized controlled trial (RCT) provides definitive evidence that initiating pravastatin in late life does not prevent or decelerate cognitive decline over a 3-year period. Despite successfully reducing cardiovascular events in this population, the lipid-lowering therapy had no impact on various cognitive domains, including executive function, processing speed, or memory. For the busy clinician, these results suggest that while statins remain vital for cardiovascular risk management in the elderly, their prescription for the sole purpose of “saving the brain” from age-related decline is futile.
Results in Context
- Primary Outcome: No significant difference in cognitive decline was found between the pravastatin and placebo groups across any cognitive domain after a mean follow-up of 42 months (all p > 0.05).
- Neuropsychological Performance: * Executive Function/Attention: Measured by the Stroop-Colour-Word test (p = 0.34).
- Processing Speed: Measured by the Letter-Digit Coding Test (p = 0.99).
- Memory: Measured by the 15-Picture Learning Test for both immediate recall (p = 0.34) and delayed recall (p = 0.91).
- Definition of Statistical Term: The interaction term of time with treatment was the primary variable of interest; a non-significant p value indicates that the rate of change (slope) in cognitive scores over 42 months did not differ between the treatment and placebo arms.
- Harms and Adverse Events: The study reports that pravastatin treatment was generally well-balanced at baseline, and while the paper focuses on cognitive outcomes, it notes that the treatment “did not affect cognitive decline,” implying no significant detrimental cognitive side effects were observed compared to placebo.
Assertive Critical Appraisal
- Risk of Bias (RoB 2 Framework): Low. This is a robust, large-scale (n=5,804) multicentre randomized placebo-controlled trial. The use of repeated measurements (six time points) and linear mixed models provides high statistical precision for detecting changes over time.
- Subgroup Analyses: The authors conducted several pre-specified subgroup analyses (sex, history of vascular disease, diabetes, APOE \epsilon4 carriership, and baseline cholesterol levels). No consistent, significant differences were found, reinforcing the primary finding.
- Reporting Quality Assessment (CONSORT): High. The study describes randomization, blinding, and participant eligibility clearly . While a flow diagram is not explicitly shown in this specific sub-analysis paper, it refers to the main PROSPER manuscript for full structural details.
- Lipophilicity Limitation: The authors acknowledge that pravastatin is hydrophilic and does not cross the blood-brain barrier. However, they correctly note that their results align with the Heart Protection Study, which used simvastatin (lipophilic) and also found no cognitive benefit.
- Applicability: The results are highly applicable to elderly patients (ages 70–82) with pre-existing vascular disease or high-risk factors. However, the study cannot rule out whether statin use initiated in midlife might prevent cognitive decline in later years.
Research Objective
To investigate whether pravastatin treatment preserves cognitive function or diminishes cognitive decline in elderly individuals at high risk of vascular disease.
Study Design
A prospective, multicentre, randomized, double-blind, placebo-controlled trial. Participants were assessed at baseline and repeatedly (9, 18, 30, and ~42 months) using a battery of four validated neuropsychological tests.
Setting and Participants
- Setting: Scotland (Glasgow), Ireland (Cork), and the Netherlands (Leiden).
- Participants: 5,804 men and women aged 70–82 years with pre-existing vascular disease or high risk (smoking, hypertension, diabetes).
- Inclusion Criterion: Participants required a Mini-Mental State Examination (MMSE) score ≥ 24 at baseline to ensure they were not already significantly cognitively impaired.
Bibliographic Data
- Title: Pravastatin and cognitive function in the elderly. Results of the PROSPER study
- Authors: Stella Trompet, Peter van Vliet, Anton J. M. de Craen, Jelle Jolles, Michael B. Murphy, Ian Ford, et al.
- Journal: Journal of Neurology
- Year: 2010 (Published online 2009)
- DOI: 10.1007/s00415-009-5271-7
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.