
Comment:
Although this article is purported to be about creatine, it’s really about animal protein, as that is the sole contributor to creatine in the diet. It’s important to recognize that data on dietary creatine derived from animal protein is not equivalent to creatine supplementation, which may drive cancer metastasis.
The researchers found that animal protein intake was not adversely associated with all-cause or cardiovascular mortality and actually showed a modest 5% reduction in cancer-related mortality (HR 0.95). This is of course, not the first paper to show positive results from higher meat consumption, such as this one.
The authors of the lay out a highly plausible biochemical defense for why whole-food animal proteins could support the body against tumorigenesis. They highlight that dietary creatine plays a vital role in cellular energy metabolism, particularly within our immune infrastructure.
The hypothesis is that consistent dietary intake optimizes ATP production in macrophages and CD8+ T cells, essentially keeping the immune system’s surveillance mechanisms well-fueled to clear abnormal cells before they can establish a foothold. Furthermore, animal foods provide a dense, highly bioavailable matrix of micronutrients—like zinc, selenium, B vitamins, and essential fatty acids—that are foundational for DNA repair pathways and metabolic integrity.
The Counter-Weight: Healthy User Bias
While those cellular pathways are elegant, the epidemiologic reality is that we cannot easily decouple a lifelong habit of consuming high-quality meat and fish from a profound Healthy User Bias.
When you look at modern Western cohorts, a high-protein diet rich in fresh animal foods (as opposed to cheap, ultra-processed foods) is very often an unmeasured surrogate marker for several protective lifestyle factors:
- Socioeconomic Resilience: Regular consumption of high-quality animal proteins often correlates with higher household income, better health literacy, and superior access to healthcare services.
- Uneven Baseline Risk: As we see in the participant characteristics of these large surveys, individuals with lower meat or protein intake are frequently older, dealing with existing chronic illnesses, or facing frailty and malabsorption—baseline imbalances that naturally distort the cancer data from the start.
Ultimately, it is entirely possible that animal proteins play a positive, neutral, or supportive role in metabolic integrity. But until we have prospective data that can cleanly isolate these whole foods from the baseline lifestyle of the people eating them, we should remain in a cautious “wait and see” stance. What this data does firmly establish is that the dogmatic conventional narrative vilifying meat consumption as an inherent, primary cancer risk is built on incredibly fragile epidemiological ground.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
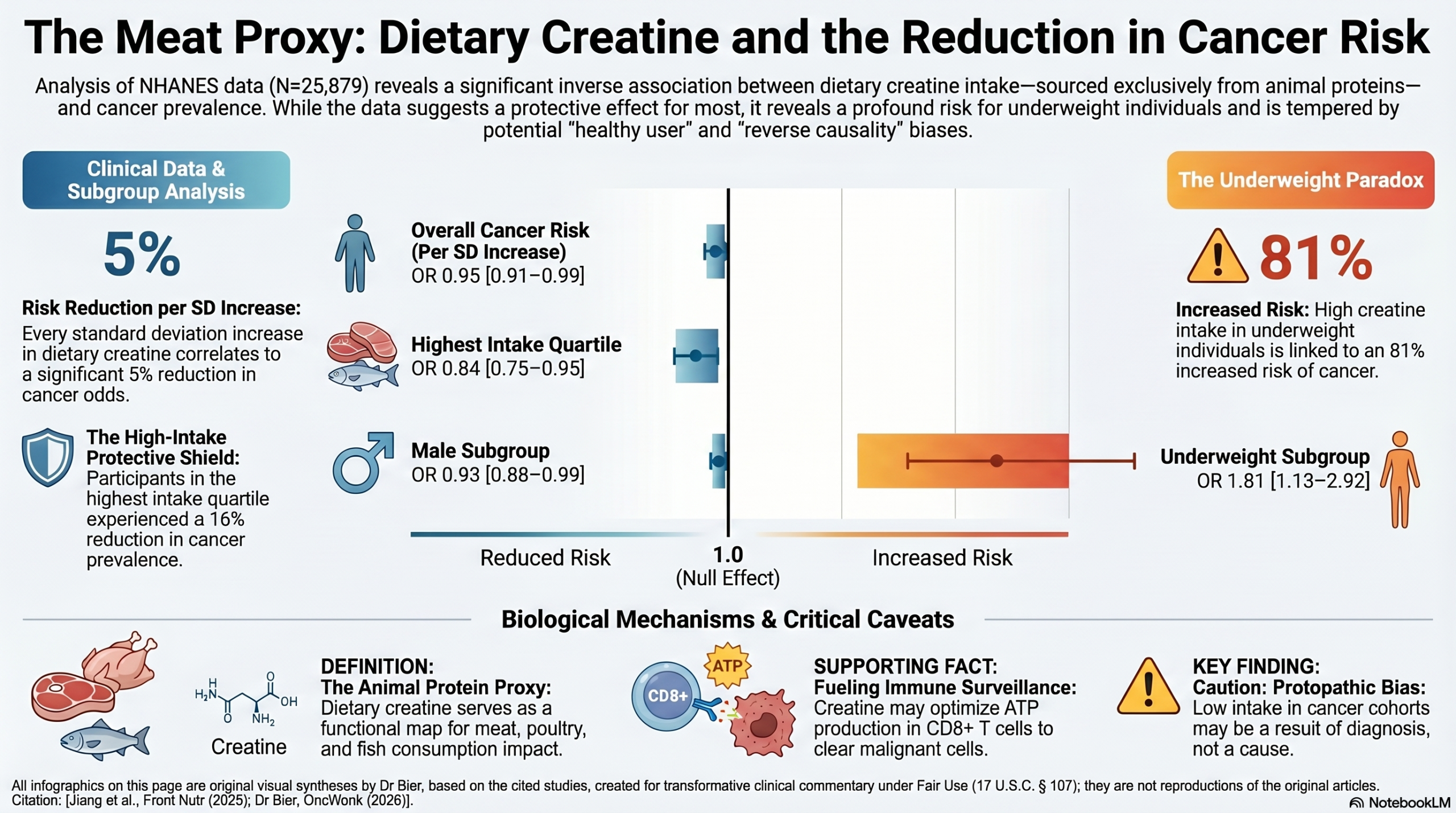
This large cross-sectional study demonstrates a significant linear inverse association between dietary creatine intake and cancer risk in U.S. adults, suggesting that higher consumption of creatine-rich foods (such as meat and fish) may provide a protective benefit against tumorigenesis. However, because this is an observational analysis relying on routinely collected real-world data and historical dietary recall, it can only establish a statistical association and cannot prove causation. Crucially, the observed “protective” association was heavily modified by baseline participant characteristics—showing a significant effect primarily in males, overweight individuals, and older populations with the highest dietary intake. , while paradoxically indicating an increased risk among underweight individuals. These nuances, combined with critical methodological limitations like mean imputation of missing data and potential recall bias, mean that these findings are hypothesis-generating and should not be used to alter clinical practice or dietary guidelines without prospective validation.
Results in Context
Main Results & Definitions
- Overall Association: Multiple logistic regression analysis adjusted for all covariates revealed a significant negative correlation between dietary creatine and cancer risk. For each standard deviation (SD) increase in continuous dietary creatine intake (SD = 0.09 g), the risk of cancer decreased by 5% (adjusted Odds Ratio [OR] = 0.95, 95% CI: 0.91–0.99, p = 0.025).
- Quartile Analysis: When categorized into quartiles of intake, participants in the highest quartile (4th quartile; mean = 0.24 ) had a 16% lower risk of cancer compared to those in the lowest quartile (1st quartile; mean = 0.03 g) with an adjusted OR = 0.84 (95% CI: 0.75–0.95, p = 0.005).
- Statistical Terms Defined for the Clinician: An Odds Ratio (OR) measures the odds of an outcome occurring in an exposed group compared to an unexposed group. An adjusted OR of 0.95 implies that for every 1 SD increase in creatine intake, the odds of a cancer diagnosis decrease by 5% after mathematically holding all other confounding variables constant. The 95% Confidence Interval (CI) represents the range within which the true population parameter is expected to lie with 95% probability; because the intervals for the primary findings exclude the value of 1.0, the results are statistically significant at the conventional 5\% level (p < 0.05).
Key Subgroup & Stratified Outcomes
- Sex Stratification: The protective association was highly pronounced and statistically significant in males (adjusted OR = 0.93 per SD increase, 95% CI: 0.88–0.99, p = 0.021), but completely disappeared and lost significance in females (adjusted OR = 0.99 per SD increase, 95% CI: 0.92–1.07, p = 0.817).
- BMI Stratification: Overweight individuals demonstrated a significant inverse correlation (adjusted OR = 0.92, 95% CI: 0.84–0.99, p = 0.044). Conversely, underweight individuals showed an opposite, detrimental trend, where higher dietary creatine intake was significantly associated with an increased risk of cancer (adjusted OR = 1.81, 95% CI: 1.13–2.92, p = 0.014).
- Age Stratification and Interaction: Restricted Cubic Spline (RCS) analysis originally showed a positive linear correlation between age and cancer risk (adjusted OR = 3.27 per SD increase, p < 0.001). Interaction testing revealed specific age-group effects (p < 0.001). Further joint association analysis demonstrated that the protective effect of creatine was heavily driven by the elderly population (ages 52–80) in the highest intake quartile, where each SD increase was linked to a 14% reduction in cancer risk (adjusted OR = 0.86, 95% CI: 0.77–0.97, p = 0.014).
Participants
- A total of 59,842 individual records were initially screened from the National Health and Nutrition Examination Survey (NHANES) 2007–2018 database. After applying exclusion criteria (including age <20 years, pregnancy, HIV status, missing database elements, and incomplete covariates), a final cohort of 25,879 participants was analyzed, consisting of 12,772 males and 13,107 females. Within this sample, 2,715 individuals were diagnosed with cancer (overall prevalence of 10.50 per 100 persons).
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Protopathic Bias / Reverse Causality: The primary methodological concern is reverse causality. Cancer survivors are frequently advised by professional organizations (e.g., the American Cancer Society) to lower their intake of red and processed meats during and after oncology treatment. Because dietary creatine in this study was derived strictly from animal proteins, the observed lower creatine intake among cancer patients may simply be a consequence of post-diagnosis lifestyle modifications rather than a true biological cause of cancer development.
- Information and Recall Bias: Dietary information was collected using two 24-hour dietary recall interviews. Self-reported dietary data are highly susceptible to recall bias and underreporting, which can introduce non-systematic measurement error and artificially attenuate or distort the true effect size.
- Omission of Key Exposures: The exposure calculation excluded non-meat protein sources and did not account for the use of external over-the-counter creatine supplements. While the supplement-using cohort is small, its omission could skew the observed protective trends. Furthermore, the analysis did not isolate the confounding benefits of other anti-cancer nutrients naturally found in animal proteins, such as Vitamin D and omega-3 fatty acids from fish.
- Inappropriate Handling of Missing Data: Missing data values were managed using sequential mean imputation. Mean imputation mathematically reduces variance, artificially narrows confidence intervals, and can severely distort or obscure true relationships between variables when data are not missing completely at random. Advanced modeling techniques, such as Bayesian multiple imputation, would have been far more methodologically sound.
Reporting Quality Assessment (STROBE)
- STROBE Compliance Audit: The authors adhered well to several core STROBE requirements by detailing a clear participant flow diagram, outlining clear eligibility cutoffs, listing extensive environmental and occupational confounders (e.g., blood cadmium, blood lead), and reporting adjusted estimates alongside crude data. However, they failed to provide a fully transparent unadjusted baseline characteristic table comparing the exact clinical profiles of the individual creatine quartiles, which is highly relevant to evaluate for residual confounding across intake tiers before multivariate modeling.
Reporting Quality Assessment (RECORD) for Real-World Evidence (RWE)
- RECORD Compliance Audit: Because this study leverages routinely collected health survey data (NHANES), RECORD guidelines apply. The authors successfully reported the exact survey data sources, the precise dates of database coverage (2007–2018), and referenced the diagnostic validation codes used to identify variables like diabetes. They adequately described database selection methods, but fell short of RECORD compliance by failing to detail how individual cancer types or stages were defined or ascertained from the self-reported survey responses, grouping all distinct malignant pathologies into a single heterogeneous “any kind of cancer” category.
Applicability
- The data source utilizes a nationally representative sample of community-dwelling U.S. adults, which gives the demographic distributions high generalizability to the general American public. However, clinical applicability to daily medicine is severely limited. Because distinct cancer types (e.g., breast, colon, lung) have entirely separate pathophysiology, grouping them into a single binary outcome prevents a clinician from applying these insights to a specific tumor type. Additionally, given the threat of reverse causality and the dangerous positive risk correlation found in underweight individuals, clinicians must not recommend increasing animal protein or creatine intake for the purpose of primary cancer prevention based on this text.
Research Methodology Profile
- Research Objective: To investigate the statistical relationship between average daily dietary creatine intake and the prevalence of cancer in a nationally representative sample of American adults.
- Study Design: Cross-sectional, population-based observational study utilizing routinely collected public health survey data.
- Setting and Participants: Non-institutionalized civilian individuals across the United States who completed the NHANES cycles between 2007 and 2018. Eligible participants were adults aged 20 years and older who possessed complete records for dietary interviews, cancer status, and all predefined confounding covariates.
Bibliographic Data
- Title: The association between dietary creatine intake and cancer in U.S. adults: insights from NHANES 2007-2018
- Authors: Junhui Jiang, Hu Zhao, Jiong Chen, Junhao Du, Weixiang Ni, Baohua Zheng, Junhong Wu, and Chunhong Xiao
- Journal: Frontiers in Nutrition
- Year: 2025
- DOI: 10.3389/fnut.2024.1460057
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.