
Comment:
The finding that 2 g/day of Grape Seed Extract (GSE) resulted in a 32.67% decrease in proteinuria and a decrease in creatinine are definitely clinically relevant outcomes. Furthermore, the significant improvements in antioxidant status (e.g., almost doubling Catalase activity) provide a plausible mechanism for the renal benefits.
The major issue is the massive risk of bias due to the tiny, imbalanced sample size (23 in GSE vs. 10 in placebo), which the authors don’t adequately explain. The discrepancy in the reported GFR significance in the results section contradicts the assertive abstract) also raises reporting quality concerns, but I expect that it was a typographical error.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
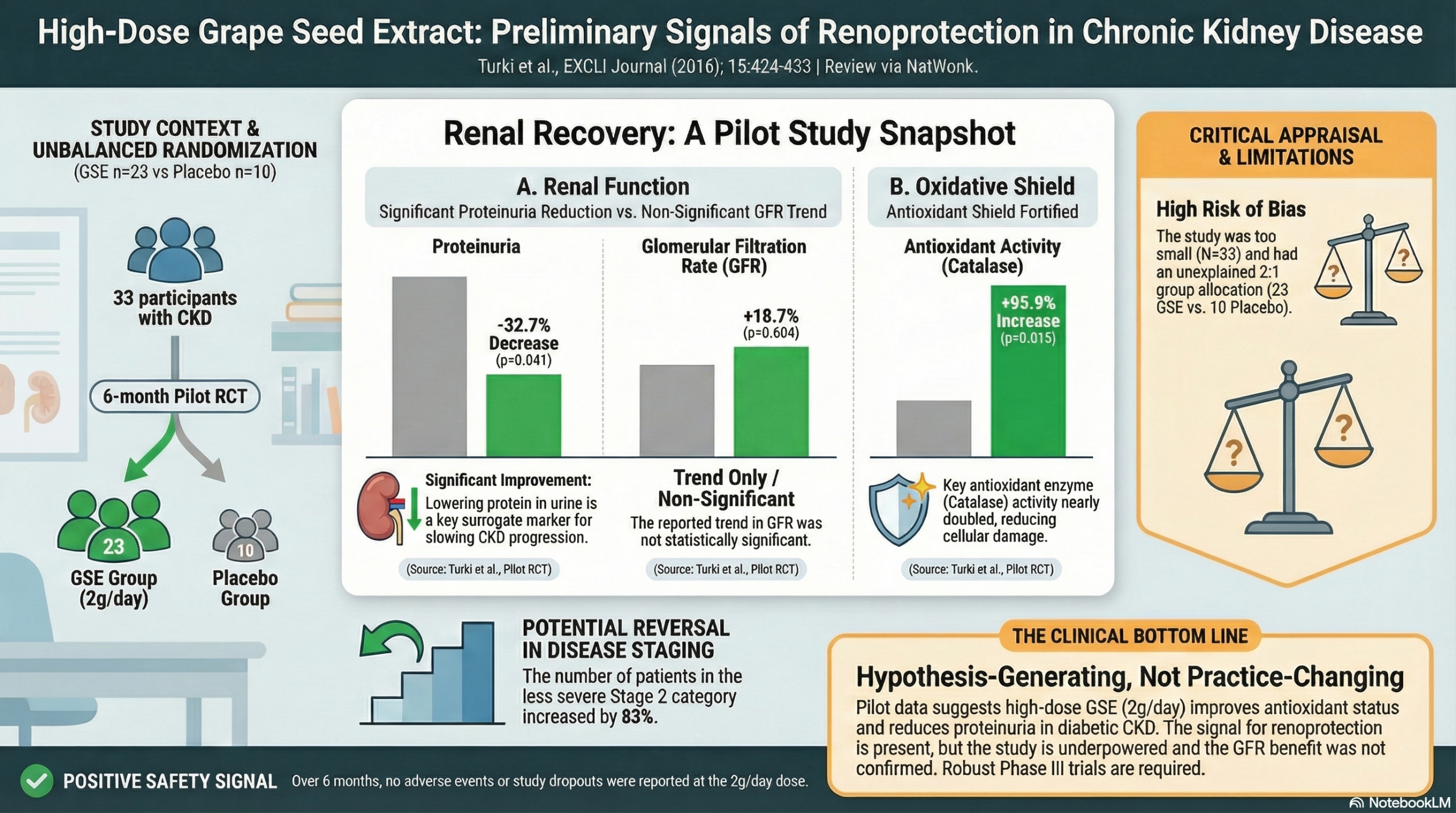
This pilot randomized controlled trial provides preliminary evidence that high-dose Grape Seed Extract (GSE) (2 g/day) may reduce proteinuria and improve antioxidant status in patients with Stage 2-4 Chronic Kidney Disease (CKD). While the authors report improvements in renal function, the study is critically limited by a very small sample size (n=33), an unexplained imbalance in group allocation (23 vs. 10), and reporting inconsistencies regarding the statistical significance of Glomerular Filtration Rate (GFR) changes. Consequently, these findings should be viewed as hypothesis-generating rather than practice-changing.
Results in Context
Primary Outcome: Renal Function Biomarkers
The study did not explicitly designate a single primary endpoint but focused on a panel of renal biomarkers.
- Proteinuria: GSE supplementation resulted in a 32.67% decrease in proteinuria after 6 months compared to baseline (p=0.041). This is a clinically relevant finding, as proteinuria reduction is a key predictor of renal protection.
- 1/Plasma Creatinine Ratio: The GSE group showed a 19.42% increase in the reciprocal of plasma creatinine (p=0.044), indicating improved clearance.
- Glomerular Filtration Rate (GFR): The authors report that GSE “slightly improved” GFR by +18.70% (36.74 \pm 5.74 to 43.62 \pm 3.68 mL/min/1.73m²); however, the text reports a non-significant p-value (p=0.604) for this specific comparison, which contradicts the assertive tone of the abstract.
- Stage Migration: The study noted a shift in disease staging: the number of Stage 4 and 3 patients decreased, swelling the ranks of Stage 2 patients by 83.33%, suggesting a regression of disease severity in the treatment group.
Key Secondary Outcomes: Oxidative Stress & Inflammation
- Antioxidant Enzymes: GSE significantly increased plasma Catalase (CAT) activity by 95.94% (p=0.015) and Superoxide Dismutase (SOD) by 25.99% (p=0.049).
- Oxidative Damage: Supplementation significantly reduced protein carbonylation by 38.82% (p=0.0319) and plasma Malondialdehyde (MDA), a marker of lipid peroxidation, by 14.96% (p=0.0307).
- Inflammation (CRP): C-Reactive Protein (CRP) decreased by 12.81% in the GSE group, whereas it increased significantly by 82.83% in the placebo group (p=0.028 for the placebo change).
Harms and Adverse Events
- The authors explicitly state that no patient dropped out of the study and no adverse side effects were noted during the clinical trial period.
Assertive Critical Appraisal
Risk of Bias (RoB 2 Framework): High
- Randomization Process: The study is described as “randomized,” yet the group allocation resulted in 23 patients in the experimental group and only 10 in the placebo group. This 2:1 ratio is not explained as a deliberate design choice (e.g., unbalanced randomization), raising concerns about the randomization method or potential undisclosed exclusions/dropouts post-randomization.
- Blinding: The study claims to be “double blind” with a starch placebo.
- Sample Size: The sample size (n=33) is very small, rendering the study underpowered to detect modest differences or confirm negative findings (Type II error).
Reporting Quality Assessment (CONSORT)
- Inconsistencies: There is a discrepancy between the text and the abstract regarding GFR. The abstract states GSE “improved glomerular filtration rate”, but the results section lists a p-value of 0.604 (non-significant) for the GFR change. However, the reciprocal creatinine change was significant (p=0.044).
- Statistical Analysis: The authors used the Kruskal-Wallis test (non-parametric). Given the baseline imbalances and small n, more robust modeling (e.g., ANCOVA adjusting for baseline GFR) would have been appropriate to account for regression to the mean.
Applicability
- The population consisted of Tunisian patients with diabetic nephropathy and hypertension.
- The intervention used a specific cultivar (Carignan) from Northern Tunisia. The dosage (2g/day) is relatively high compared to standard dietary supplements, which impacts generalizability to lower-dose commercial products.
Research Objective
To test the ability of Grape Seed Extract (GSE) to improve kidney dysfunction and oxidative status in CKD patients (Stages 2, 3, 4).
Study Design
- Design: Randomized, double-blind, placebo-controlled pilot study.
- Duration: 6 months.
- Intervention: GSE group received 2 g/day (6 capsules of 350 mg). Control group received starch placebo.
Setting and Participants
- Setting: Hemodialysis unit of the Regional Hospital of Menzel Bourguiba, Tunisia.
- Participants: 33 volunteers with CKD (Stages 2-4), all suffering from diabetic nephropathy and hypertension.
- Exclusion Criteria: Smokers and patients receiving antioxidant supplements in the previous 6 months.
Bibliographic Data
- Title: Grape Seed Powder Improves Renal Failure of Chronic Kidney Disease Patients
- Authors: Turki K, Charradi K, Boukhalfa H, Belhaj M, Limam F, Aouani E
- Journal: EXCLI Journal
- Year: 2016
- DOI:dx.doi.org/10.17179/excli2016-363
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.