
Comment:
The argument for a ‘window of opportunity’—where MHT might actually be neuroprotective if timed correctly—is compelling. However I remain cautious about broadly applying this as I tend to always consider the risk side of the equation with synthetic medications.
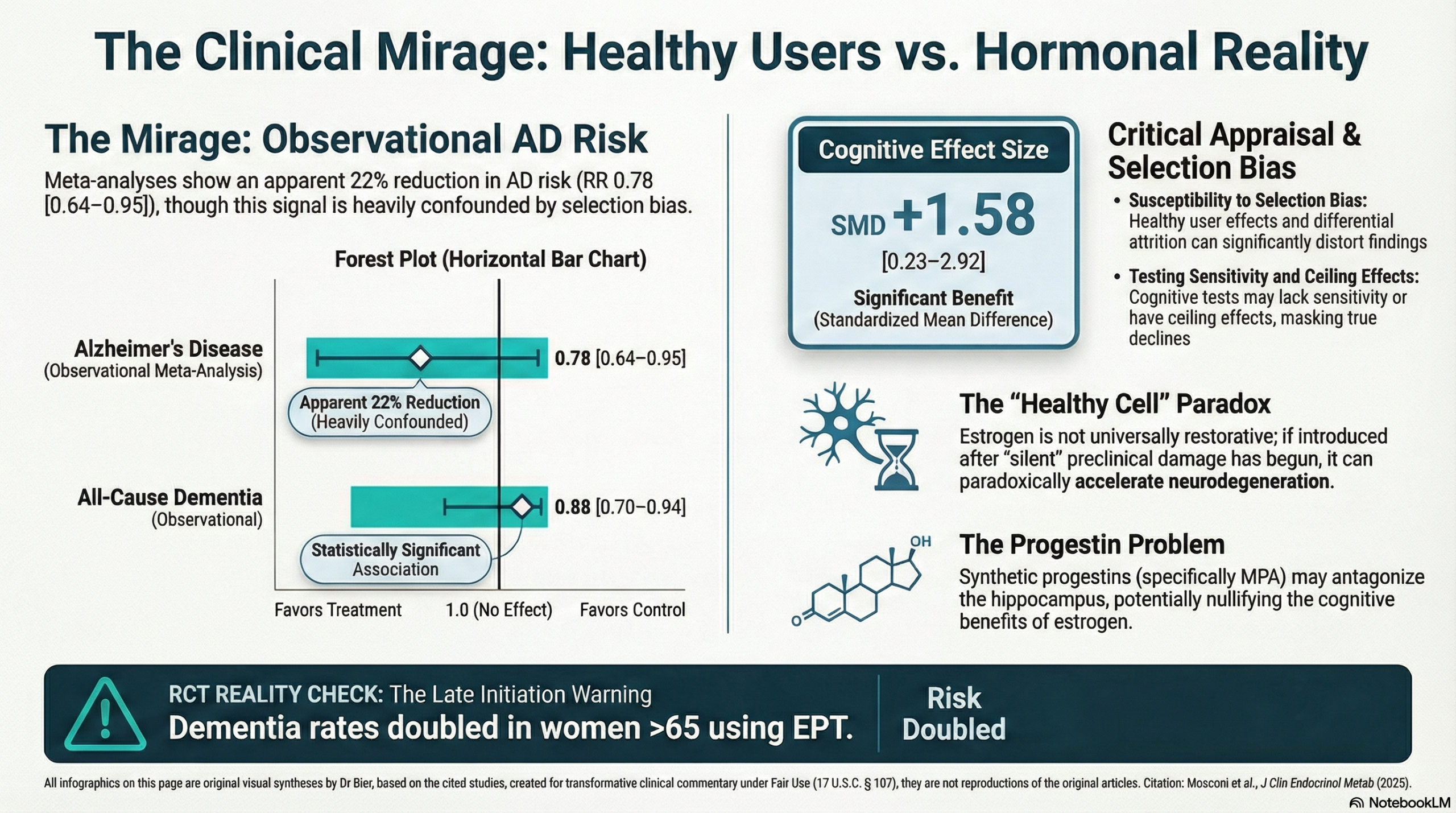
The clinical management of Alzheimer’s disease (AD) prevention has long operated on the assumption that hormonal replacement is a restorative necessity, yet this comprehensive review exposes a profound disconnect between biochemical promise and systemic biological reality. The argument for a “window of opportunity”—where menopausal hormone therapy (MHT) might be neuroprotective if initiated during a narrow midlife window—is compelling, but we must recognize that this is confounded by the “healthy-user effect”. The move away from objective randomized data toward a reliance on observational evidence may fundamentally mask the real data.
A primary concern with the observational studies suggesting a reduced risk of AD is their extreme susceptibility to selection bias and the healthy-user effect, which can distort outcomes and inflate the perceived efficacy of the conventional treatments. Women who initiate MHT in midlife often possess more favorable baseline metabolic and lifestyle profiles, creating a clinical mirage of neuroprotection. When we prioritize hard clinical endpoints over mechanistic theories, the iatrogenic legacy of the conventional standard-of-care becomes clear. Data from the Women’s Health Initiative Memory Study (WHIMS) showed that dementia rates doubled in women aged 65 and older treated with estrogen-progestogen therapy, while the Cache County data identified a 2.1-fold increased risk of AD when initiation occurred after age 61. This risk is compounded by the use of synthetic progestins like medroxyprogesterone acetate (MPA), which may specifically antagonize the memory structures of the hippocampus. We must also acknowledge the “healthy cell bias,” where exogenous estrogen can paradoxically worsen established neuropathology if introduced after preclinical damage is already present.
Prioritizing the structural integrity of the brain requires us to acknowledge that the “healthy cell bias” of estrogen can paradoxically worsen established neuropathology if introduced after preclinical damage is already present. To label any dose or route as “safe” for neuroprotection is a clinical misnomer, especially when synthetic progestins like medroxyprogesterone acetate (MPA) may specifically antagonize the memory structures we seek to preserve. The definitive takeaway is that menopause is not a deficiency state that can be “fixed” without a measurable price; any cognitive benefit is possibly secondary to baseline metabolic health rather than the hormonal intervention itself.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This narrative review argues that the relationship between Menopausal Hormone Therapy (MHT) and Alzheimer’s Disease (AD) is strictly time-dependent. While acknowledging that the Women’s Health Initiative Memory Study (WHIMS) demonstrated an increased risk of dementia when MHT is initiated in women aged 65 and older, the authors contend this finding does not apply to midlife initiation. They propose a “window of opportunity” where MHT may be neuroprotective, but emphasize that starting therapy late, or using specific synthetic formulations (medroxyprogesterone acetate), may accelerate neurodegeneration or nullify benefits.
Key Themes & Risk Analysis
1. Scope of the Review
The authors review the pathophysiology of AD as it relates to female endocrine aging, critique the generalizability of the WHIMS trial data to younger women, and advocate for a precision medicine approach that considers timing, formulation, and biomarkers.
2. Analysis of Potential Risks of MHT
Per your request, this analysis isolates the specific risks associated with MHT as detailed in the review:
- Risk of Late Initiation (The “Timing Hypothesis”): The review presents strong evidence that MHT initiated in late life (typically >65 years or >10 years post-menopause) is associated with adverse cognitive outcomes.
- In the WHIMS RCT, women aged 65+ treated with Estrogen-Progestogen Therapy (EPT) saw a doubling in dementia rates.
- Observational data from the Cache County study showed that MHT usage after age 61 was associated with a 2.1-fold increased risk of AD.
- Mechanism of Harm: The authors cite the “healthy cell bias hypothesis,” suggesting that while estrogen benefits healthy neural tissue, it may worsen established neuropathology if introduced after damage (such as clinically silent AD pathology) is already present.
- Risks Associated with Formulation (Synthetic Progestins):
- The review suggests that the specific progestogen used in WHIMS—medroxyprogesterone acetate (MPA)—may be a driver of risk.
- Evidence indicates MPA may antagonize the beneficial effects of estrogen on memory structures like the hippocampus.
- The review implies that the increased dementia risk seen in WHIMS EPT arms might be specific to the conjugated equine estrogen (CEE) + MPA combination, rather than estrogen alone or regimens using micronized progesterone.
- Genetic Risk Interaction (APOE-4):
- The review highlights that the APOE-4 allele increases AD risk more significantly in women than in men.
- While some data suggests MHT might reduce amyloid load in APOE-4 carriers, the review notes that including both high-risk and low-risk groups in studies without stratification may obscure specific risks or benefits.
- General Medical Risks:
- The authors acknowledge standard MHT-associated risks, including breast cancer, stroke, and venous thromboembolism.
- However, they contextualize this by stating these events are generally considered rare ($<$10 events per 10,000 women) when therapy is initiated in women under 60 or within 10 years of menopause.
Assertive Critical Appraisal
- Evidence Level: Level 5 (Narrative Review/Expert Opinion). This is a mini-review summarizing existing literature rather than a systematic meta-analysis or original trial.
- Quality Assessment (SANRA Scale):
- Justification & Aims: The review clearly defines its aim to re-evaluate MHT as a preventive strategy for AD in the context of new biomarker definitions.
- Literature Search: Flag: The authors do not describe their search strategy, keywords, or inclusion/exclusion criteria. This makes the review susceptible to selection bias, as the authors may have prioritized studies that support the “window of opportunity” hypothesis while potentially excluding contradictory data.
- Scientific Reasoning: The argument is logically constructed, effectively contrasting the “healthy cell bias” against the results of the WHIMS trial. The distinction between chronological aging and endocrine aging is well-supported by the cited pathophysiology.
- Data Presentation: The review relies on summarizing findings from other studies (WHIMS, KEEPS, ELITE). It appropriately acknowledges the limitations of using cognitive test scores in younger, high-functioning cohorts (ceiling effects).
Research Objective
The objective of this review is to examine MHT as a female-specific, time-sensitive therapy for the reduction of AD and dementia risks, and to argue for the use of AD biomarkers (neuroimaging and fluid) as endpoints in future clinical trials.
Bibliographic Data
- Title: New Horizons in Menopause, Menopausal Hormone Therapy, and Alzheimer’s Disease: Current Insights and Future Directions
- Authors: Mosconi L, Nerattini M, Williams S, Fink M.
- Journal: The Journal of Clinical Endocrinology & Metabolism
- Year: 2025
- DOI: 10.1210/clinem/dgaf026
Original Article:
Full text:
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.