
Comment:
It is always important the acknowledge the risks in observational studies, however when the results keep coming back the same, it is important to pay attention. The Core Tension in the current discourse on metabolic health is the friction between the popularized biochemical “panacea” of intermittent fasting and the sobering mortality signals emerging from large-scale human models. While mechanistic studies often highlight short-term weight loss or improved insulin sensitivity to justify skipping breakfast, this meta-analysis of 2,383,813 participants provides a necessary corrective, prioritizing hard clinical endpoints over theoretical metabolic shifts. Theoretical gains in surrogate markers do not override a mortality signal this strong in actual humans.
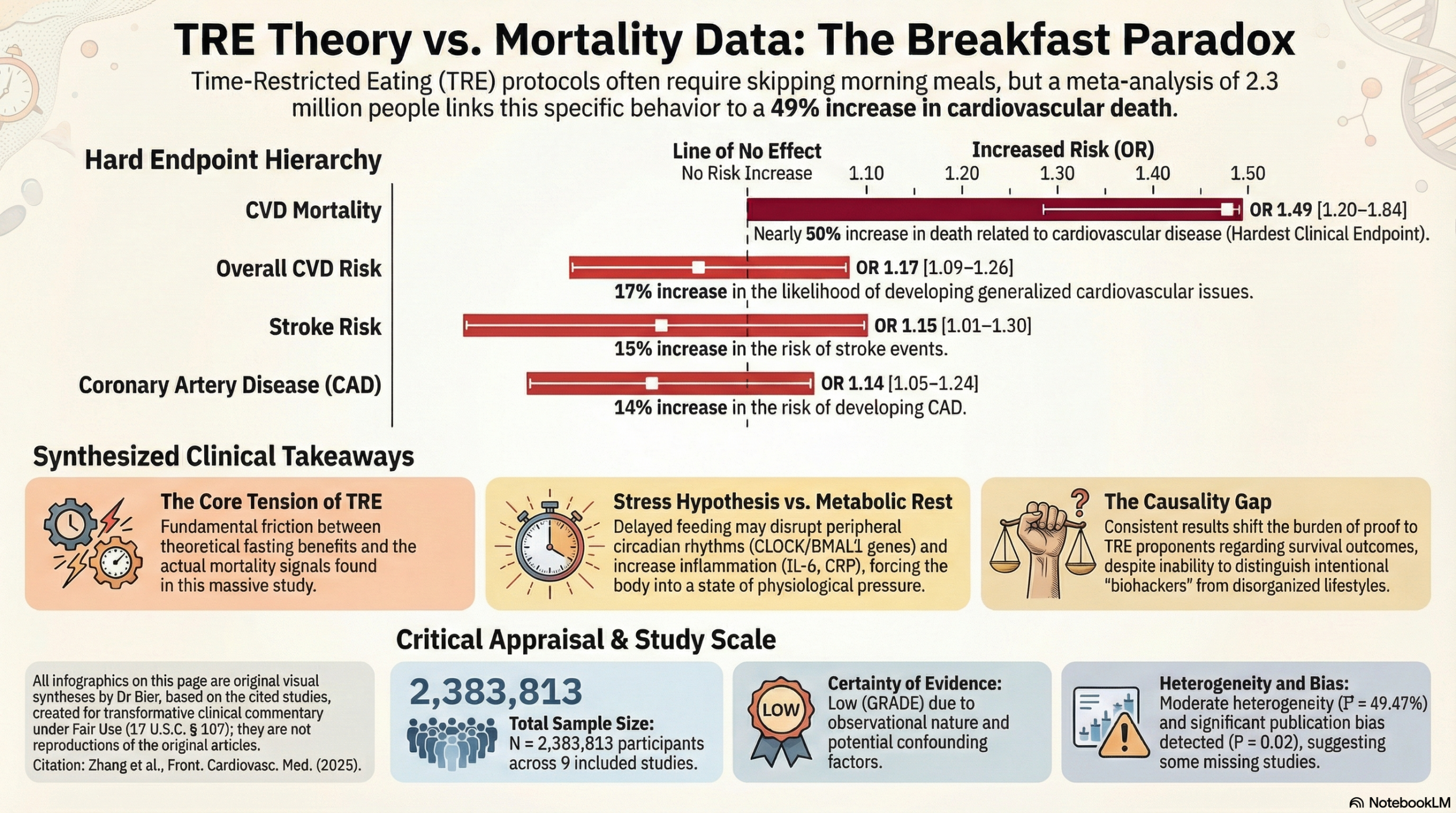
The data reveals a consistent and alarming association between breakfast skipping and an escalation in hard outcomes:
-
Cardiovascular Mortality: The most critical finding is a 49% increase in cardiovascular disease mortality.
-
Heart and Brain Risk: Beyond survival, the risk of developing specific disease is persistent, showing a 17% increase in overall CVD risk, a 14% increase in coronary artery disease, and a 15% increase in stroke risk.
The proposed mechanisms—disruption of peripheral circadian rhythms and resulting chronic inflammation—offer a compelling counter-narrative to the standard Time-Restricted Eating (TRE) defense. If forgoing the morning meal forces the body into a state of physiological pressure that overrides the “benefits” of a longer fasting window, then the metabolic health gained is merely a secondary metric masking a primary harm. We must treat any protocol that influences human survival as a serious intervention that must prove its worth. Until high-quality human clinical models demonstrate that intentional morning fasting improves overall survival, I urge caution.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
This meta-analysis of observational studies suggests that skipping breakfast—a behavior often inherent to Time-Restricted Eating (TRE) protocols like the 16:8 method—is significantly associated with an increased risk of cardiovascular disease (CVD), coronary artery disease (CAD), stroke, and cardiovascular mortality. While this data highlights potential cardiovascular risks associated with prolonged fasting windows that exclude morning meals, the certainty of this evidence is rated as Low. This is due to the observational nature of the included studies (unable to prove causation), the inability to distinguish between intentional TRE and disorganized eating habits, and the detection of significant publication bias.
Results
- Summary of Results: The analysis included 9 studies comprising 2,383,813 participants. The pooled analysis showed that skipping breakfast was associated with a statistically significant increase in adverse cardiovascular outcomes compared to regular breakfast consumption:
- Overall CVD Risk: OR 1.17 (95% CI: 1.09-1.26).
- Coronary Artery Disease (CAD): OR 1.14 (95% CI: 1.05-1.24).
- Stroke: OR 1.15 (95% CI: 1.01-1.30).
- Cardiovascular Disease Mortality (CDM): OR 1.49 (95% CI: 1.20-1.84).
Assertive Critical Appraisal
- Certainty of Evidence (GRADE Framework): Low. The evidence is derived principally from observational cohort and cross-sectional studies. While the authors rated the individual studies as “high quality” using the Newcastle-Ottawa Scale, observational data regarding diet is highly susceptible to unmeasured confounding (e.g., lifestyle factors, socioeconomic status) and recall bias.
- Relevance to Time-Restricted Eating (TRE):
- Confounding of “Skipping”: The study defines skipping breakfast simply as “consuming breakfast less than five times a week or not at all”. It does not distinguish between patients practicing intentional, health-conscious TRE and those skipping breakfast due to poor sleep, stress, or chaotic lifestyles. Therefore, the “risks of TRE” inferred here may actually reflect the risks of a generally unhealthy lifestyle associated with breakfast omission in the general population.
- Physiological Mechanisms of Risk: The authors propose specific mechanisms for why skipping the morning meal (and by extension, delayed eating windows in TRE) may carry risk:
- Circadian Disruption: Delayed feeding may disrupt peripheral circadian rhythms and the expression of clock genes (CLOCK, BMAL1) involved in lipid metabolism, potentially leading to dyslipidemia.
- Glucose & Insulin Dysregulation: Morning fasting was associated with impaired insulin sensitivity and glucose intolerance.
- Inflammation: Habitual skipping is linked to elevated pro-inflammatory mediators (C-reactive protein, IL-6) which are correlated with hypertension and arterial stiffness.
- Heterogeneity: The analysis showed moderate heterogeneity for the overall CVD outcome (I2 = 49.47%). This I2 value indicates that nearly 50% of the variation across studies is due to real differences (population, definition of skipping, follow-up time) rather than chance, suggesting the pooled average should be interpreted with some caution. Notably, heterogeneity was high for stroke (I2 = 63.47%), indicating inconsistent findings across the specific stroke studies.
- Publication Bias: The authors detected significant publication bias using Egger’s test (P = 0.02). This suggests that smaller studies with negative results (showing no harm from skipping breakfast) may be missing from the literature, potentially leading to an overestimation of the cardiovascular risk reported here. Although a “trim and fill” analysis was used to theoretically correct this, the presence of bias remains a concern.
- Subgroup Analyses: The association between skipping breakfast and CAD weakened and became non-significant in studies with fewer than 10,000 participants or follow-up periods under five years. This suggests the cardiovascular harm may be a long-term process that requires large datasets to detect.
- Reporting Quality Assessment (PRISMA): The study generally adheres to PRISMA guidelines, providing a flow chart of study selection and registering the protocol with PROSPERO.
- Applicability: The results are relevant to general practice but should be applied cautiously to patients asking about TRE. While the data suggests a signal of harm for skipping breakfast, it is drawn from Western and Asian general populations and may not fully apply to a patient engaging in a monitored, high-quality nutritional TRE program.
Research Objective: To clarify the relationship between skipping breakfast and cardiovascular disease (CVD) through a systematic review and meta-analysis of prospective research.
Study Design: Systematic review and meta-analysis of 9 observational studies (8 cohort, 1 cross-sectional).
Setting and Participants: The analysis included 2,383,813 participants. Studies were conducted in the US, Japan, and India.
Bibliographic Data:
- Title: The association between skipping breakfast and cardiovascular disease a meta analysis
- Authors: Zhang H, Zhang S, Liu Y, Wang X, Hu J
- Journal: Frontiers in Cardiovascular Medicine
- Year: 2025
- DOI: 10.3389/fcvm.2025.1565806
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.