
Comment:
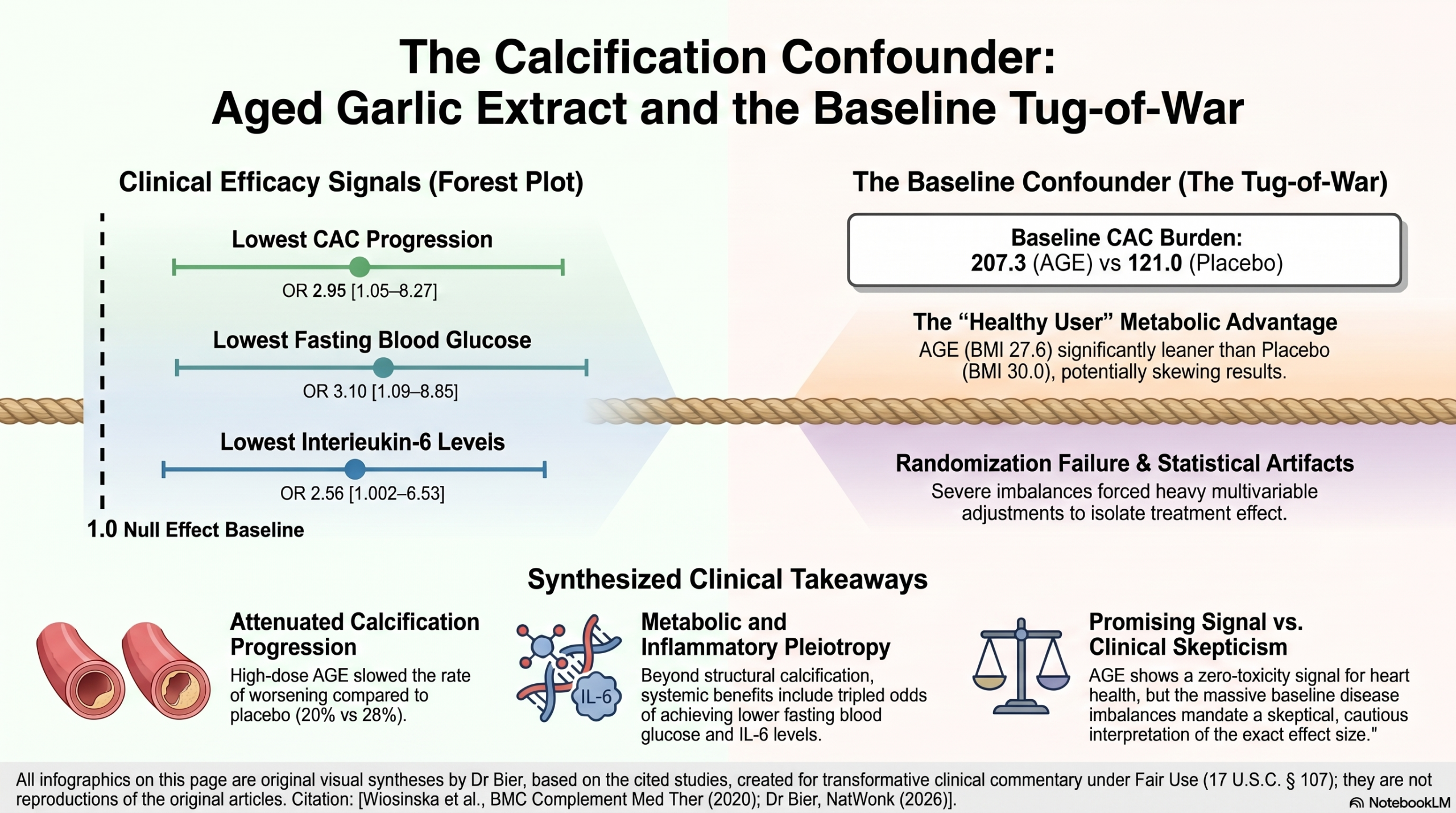
I use Aged Garlic Extract in my practice for plaques and calcifications as there are no risks to offset the potential benefit. But I do need to apply the same standards to the study as I do to a statin trial. This data reveals presents a conflicting baseline that muddies any clear clinical conclusion. On one hand, the AGE group possessed a clear Healthy User advantage by being significantly leaner than the placebo group (BMI 27.6 vs. 30.0; p=0.01). Conversely, that same AGE group started with nearly double the initial calcification burden (207.3 vs. 121.0). This creates a statistical “tug-of-war” where we are forced to weigh a metabolic head-start against a more advanced disease state. When a study requires such heavy multivariable lifting to “equalize” these disparate starting points, the reported 2.95 odds of success may be a statistical artifact rather than a biological certainty.
And since there is no risk, and other supportive studies, I will continue to use it.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This study suggests that 2400 mg of Aged Garlic Extract (AGE) daily significantly inhibits the progression of coronary artery calcification (CAC) and improves metabolic markers (glucose, IL-6, and systolic blood pressure) in European patients with intermediate-to-high cardiovascular risk. While the findings are promising—showing a 2.95 times higher probability of reduced CAC progression in the treatment group—the study is limited by significant baseline imbalances. Specifically, the AGE group started with higher initial calcium scores and LDL cholesterol levels than the placebo group, which complicates the interpretation of the results despite statistical adjustments.
Results in Context
Primary Outcome
- CAC Progression: The primary endpoint was the change in CAC score over 12 months.
- Result: The probability of belonging to the group with the lowest CAC progression was 2.95 times higher in the AGE group compared to placebo (adjusted OR: 2.95 [1.05–8.27], p=0.040).
- Definition: CAC progression was measured using the Agatston score via cardiac CT. While both groups saw an increase in calcification, the AGE group’s progression was 20% compared to 28% in the placebo group.
Key Secondary Outcomes
- Blood Glucose: The AGE group had a 3.1 times higher probability of having lower glucose levels (adjusted OR: 3.1 [1.09–8.85], p=0.034).
- Inflammation (IL-6): The probability of having the lowest IL-6 (a marker of vascular inflammation) was 2.56 times higher in the AGE group (adjusted OR: 2.56 [1.002–6.53], p=0.049).
- Blood Pressure: Systolic blood pressure in the AGE group decreased significantly from a mean of 148 mmHg to 140 mmHg (p=0.027), while no significant change was observed in the placebo group.
Harms and Adverse Events
- Tolerability: There were no side effects reported in either the active or placebo groups.
- Safety Profile: AGE was noted for its high tolerability and high safety profile as a dietary supplement.
Assertive Critical Appraisal
Risk of Bias (RoB 2 Framework)
Judgment: Some Concerns.
- Baseline Imbalance (Critical Issue): Despite randomization, there were significant differences between the two groups at the start of the study.
- The AGE group had a significantly higher baseline CAC score (mean 207.3 vs 121.0) and higher LDL cholesterol (mean 3.4 vs 2.9 mmol/L).
- The placebo group had a significantly higher BMI (mean 30.0 vs 27.6).
- Impact on Outcome: Starting with higher CAC and LDL levels typically suggests more advanced disease, which might naturally progress at a different rate than earlier-stage disease. While the authors used multivariable logistic regression to “equalize” these differences, such imbalances suggest the randomization may not have perfectly distributed confounders, potentially skewing the effect size.
Predictive Modeling (AGE Algorithm)
- The authors used CRISP-DM (data mining) to create a predictive algorithm.
- Finding: The model predicted CAC progression with 80% precision.
- Critique: While innovative, this is a proof-of-concept analysis with a small sample size (n=46 for training/testing via leave-one-out cross-validation). These results are exploratory and must be validated in larger, independent cohorts before clinical use.
Reporting Quality Assessment (CONSORT)
- Strengths: The study included a CONSORT flow diagram, clearly showing enrollment, allocation, and follow-up.
- Randomization/Blinding: Methods were adequate, utilizing a computer-generated chart and numbered containers to maintain the double-blind status.
Applicability
- The study is highly relevant to European populations with intermediate-to-high cardiovascular risk, a group previously under-represented in garlic research.
Research Objective
To evaluate whether aged garlic extract (AGE) can influence the rate of coronary artery calcification (CAC) and to create a predictive algorithm for its individual effects.
Study Design
- Type: Single-center, parallel, randomized, double-blind, placebo-controlled study.
- Duration: 12 months.
- Participants: 104 randomized (52 per group); 93 completed the analysis (47 placebo, 46 AGE).
Setting and Participants
- Setting: University hospital in Lund, Sweden (October 2016 – October 2018).
- Inclusion Criteria:
- Asymptomatic patients aged 40–75 years.
- Framingham risk score ≥10.
- Positive CAC score on cardiac CT.
- Stable medications for ≥4 months; if diabetic, HbA1c < 8.0 and stable for 6 months.
- Exclusion Criteria: Included history of MI, symptoms of ischemic heart disease, CAC > 1000 units, and severe hypertension (> 170/110 mmHg).
Bibliographic Data
- Title: The effect of aged garlic extract on the atherosclerotic process – a randomized double-blind placebo-controlled trial.
- Authors: Wlosinska M, Nilsson A-C, Hlebowicz J, et al..
- Journal: BMC Complementary Medicine and Therapies.
- Year: 2020.
- DOI: https://doi.org/10.1186/s12906-020-02932-5.
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.