
Comment:
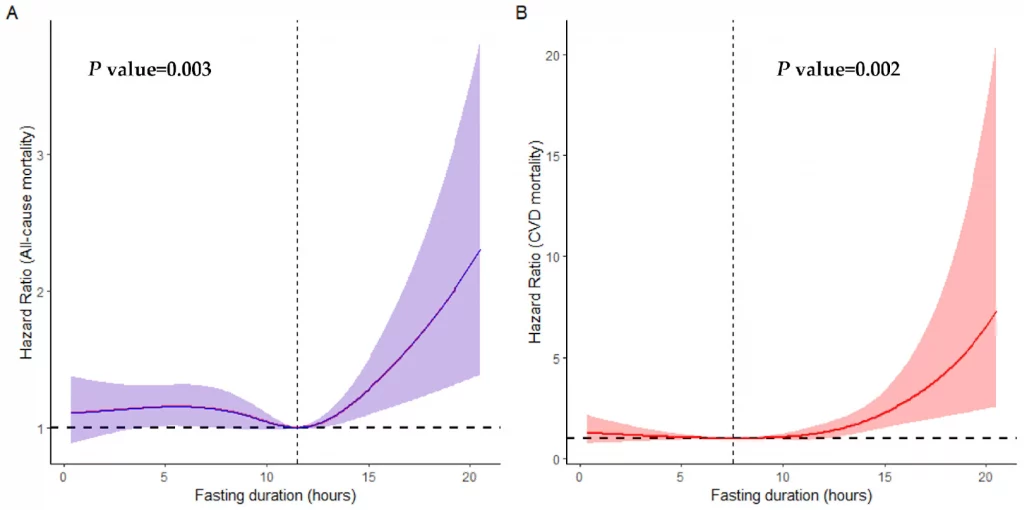
This is another large-scale analysis to flag a mortality signal, giving sufficient reason to move the discussion from a “statistical fluke” to a “clear clinical pattern.” There is often a linear assumption—that if a 12-hour fast is good, 16 hours must be better. However, this US-based cohort study of over 10,000 elderly adults forces us to confront a biological reality: physiology is rarely linear; it is almost always U-shaped.
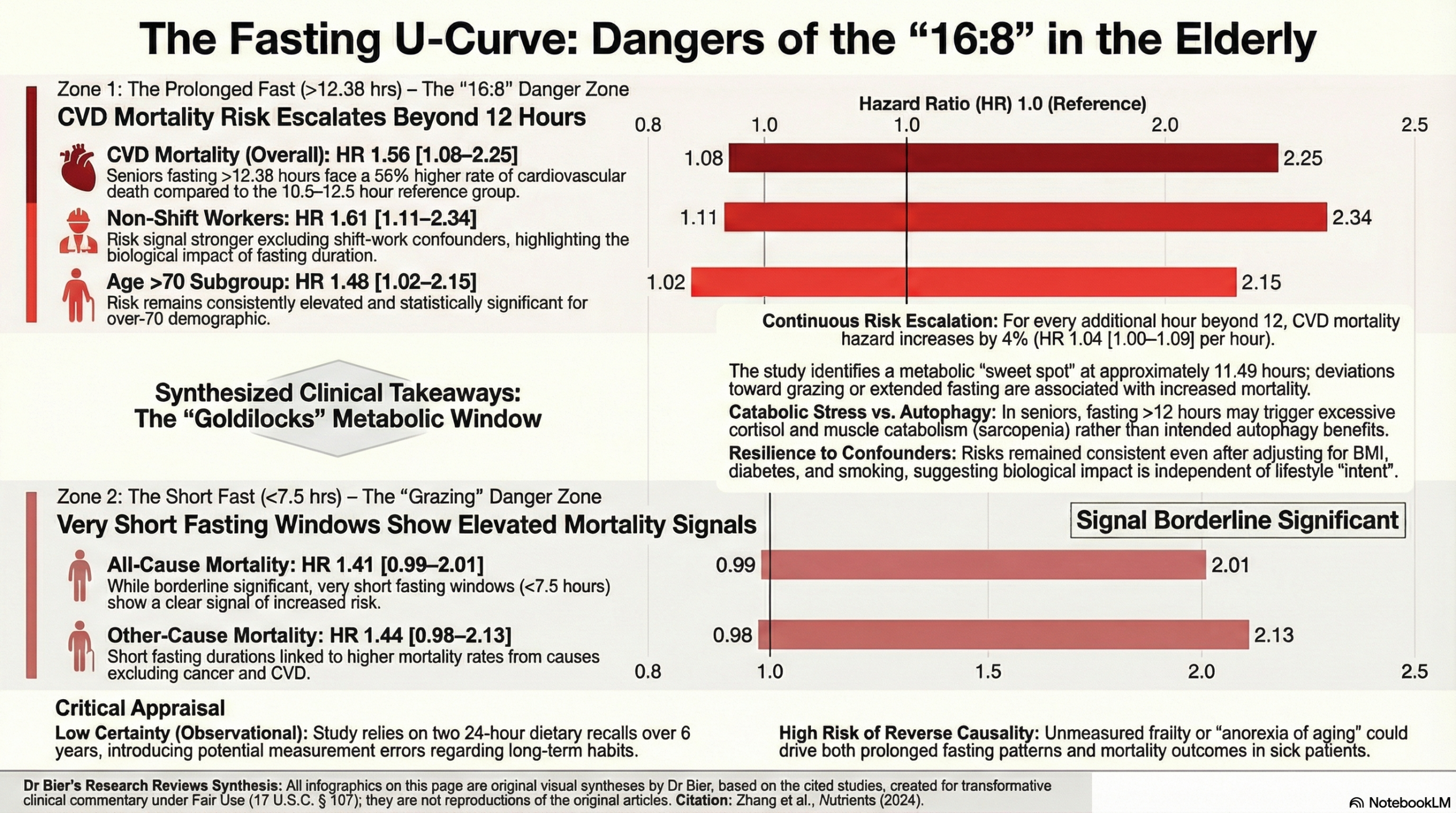
The data here is specific and sobering for the geriatric population. Rather than looking at generic “meal skipping,” the authors pinpointed a precise threshold where risk begins to escalate. The finding that fasting beyond just 12.38 hours is associated with a 56% increase in cardiovascular mortality (HR 1.56) directly challenges the safety of standard “16:8” protocols for older adults. The theoretical benefits of deep autophagy appear to be outweighed by the tangible risks of frailty and cardiovascular stress when applied to aging bodies.
Proponents of fasting often dismiss these observational findings by claiming they capture “unintentional” starvation rather than “therapeutic” fasting. While intent is a valid variable, biology is the ultimate arbiter. The authors rightly identify potential mechanisms—specifically muscle catabolism and cortisol elevation—that make prolonged fasting uniquely hazardous for the elderly. The discovery of a “Goldilocks zone” at approximately 11.5 hours suggests that for patients over 60, metabolic health is found in balance, not extremes.
The consistent signal across multiple studies suggests that aggressive fasting regimens may act as a catabolic stressor rather than a longevity aid in older populations. Until randomized trials prove otherwise, the burden of proof is on showing long-term positive outcomes.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
This prospective cohort study of over 10,000 U.S. elderly adults suggests a U-shaped relationship between overnight fasting duration and mortality. Crucially, the study identifies a significant risk associated with prolonged fasting: individuals over age 60 who fasted for longer than 12.38 hours per night had a significantly increased risk of cardiovascular disease (CVD) mortality compared to those with a “normal” fasting duration (approx. 10.5–12.5 hours). This risk was most pronounced in patients over 70 and those with cardiovascular comorbidities. Conversely, very short fasting durations (<7.5 hours) were associated with increased cancer and other-cause mortality. While Time-Restricted Eating (TRE) is often promoted for metabolic health, this observational data suggests clinicians should exercise caution before recommending aggressive fasting regimens (>12 hours) to elderly patients, as the lowest mortality risk was observed at a fasting duration of approximately 11.5 hours.
Results in Context
- Main Results (The Risks of Prolonged Fasting):
- CVD Mortality: When comparing the longest fasting group (>12.38 hours) to the reference group (10.58–12.38 hours), prolonged fasting was associated with a Hazard Ratio (HR) of 1.56 (95% CI: 1.08–2.25) for CVD mortality.
- Subgroup Risks: The elevated risk of CVD mortality in the prolonged fasting group was specifically significant in:
- Non-shift workers: HR 1.61 (95% CI: 1.11–2.34).
- Individuals aged >70 years: HR 1.48 (95% CI: 1.02–2.15).
- Continuous Variable Analysis: For every 1-hour increment in fasting duration, there was a 4% increase in the hazard of CVD mortality (HR 1.04, 95% CI: 1.00–1.09).
- Main Results (The Risks of Short Fasting):
- Cancer & Other-Cause Mortality: The shortest fasting group (<7.5 hours) showed elevated risks for all-cause mortality (HR 1.41) and other-cause mortality (HR 1.44), though the p-values were just above the significance threshold of 0.05.
- Definitions:
- Hazard Ratio (HR): An HR of 1.56 indicates that, at any given time point during the study, the group fasting >12.38 hours had a 56% higher rate of dying from cardiovascular disease compared to the reference group.
- Fasting Duration: Calculated by subtracting the time between the first and last caloric intake from 24 hours.
- Participants:
- The analysis included 10,561 elderly participants (mean age 69.89 years) tracked over a median follow-up of 6.66 years.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework):
- Recall Bias & Measurement Error: The exposure (fasting duration) was determined based on only two 24-hour dietary recalls. This is a major limitation, as it assumes these two days are representative of the participants’ long-term lifestyle habits over nearly 7 years of follow-up. It is highly possible that eating windows fluctuated significantly.
- Reverse Causality: This is a critical consideration in observational geriatrics. The study notes that prolonged fasting was associated with higher rates of diabetes, CVD, hypertension, and depression at baseline. It is plausible that sicker, frailer patients were naturally eating less or fasting longer due to illness (anorexia of aging) or medication schedules, rather than the fasting causing the mortality. While the authors adjusted for these comorbidities, residual confounding remains a strong possibility.
- Lack of Intent: Most participants likely were not practicing intentional “Time-Restricted Eating” (TRE) as a health intervention, as the data predates the mainstream popularity of TRE (2017–2018). Therefore, the results reflect habitual eating patterns rather than the effects of a structured clinical intervention.
- Reporting Quality Assessment (STROBE):
- Confounding: The authors utilized rigorous multivariable Cox proportional hazards models, adjusting for a wide range of variables including age, gender, ethnicity, BMI, smoking, diabetes, and dietary inflammatory index. This strengthens the validity of the association, even if causation cannot be proven.
- Missing Data: The study clearly reports excluding 2,906 participants due to missing dietary data, which is a standard approach but could introduce selection bias if those with missing data were systematically different (e.g., too frail to complete the recall).
- Applicability:
- The findings are highly applicable to US geriatric practice as the data is derived from NHANES, a nationally representative survey. The results suggest a “Goldilocks” window for eating in the elderly: avoiding both very short eating windows (prolonged fasting) and very long eating windows (short fasting).
Research Objective: To examine the correlation between fasting duration and mortality within a nationally representative cohort of elderly individuals (aged over 60) in the United States.
Study Design: Prospective cohort study using data from the National Health and Nutrition Examination Survey (NHANES) 2005–2018, linked to the National Death Index through December 31, 2019.
Setting and Participants:
- Setting: United States (National Survey data).
- Participants: 10,561 community-dwelling adults aged over 60 years who had complete dietary intake and mortality follow-up data.
Bibliographic Data:
- Title: A National Study Exploring the Association between Fasting Duration and Mortality among the Elderly
- Authors: Zhang Z, Zhao H, Tao Z, Jiang M, Pu J.
- Journal: Nutrients
- Year: 2024
- DOI: https://doi.org/10.3390/nu16132018
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.