
Comment:
This study shifted my thinking around nattokinase as it somewhat clarified contradictions in the literature around efficacy, specifically it showed the failure of the “standard” 2,000 FU recommendation to hit the physiological threshold necessary for vascular remodeling. This study of 1,062 participants suggests that biology requires far more significant saturation to move the needle on established carotid plaque.
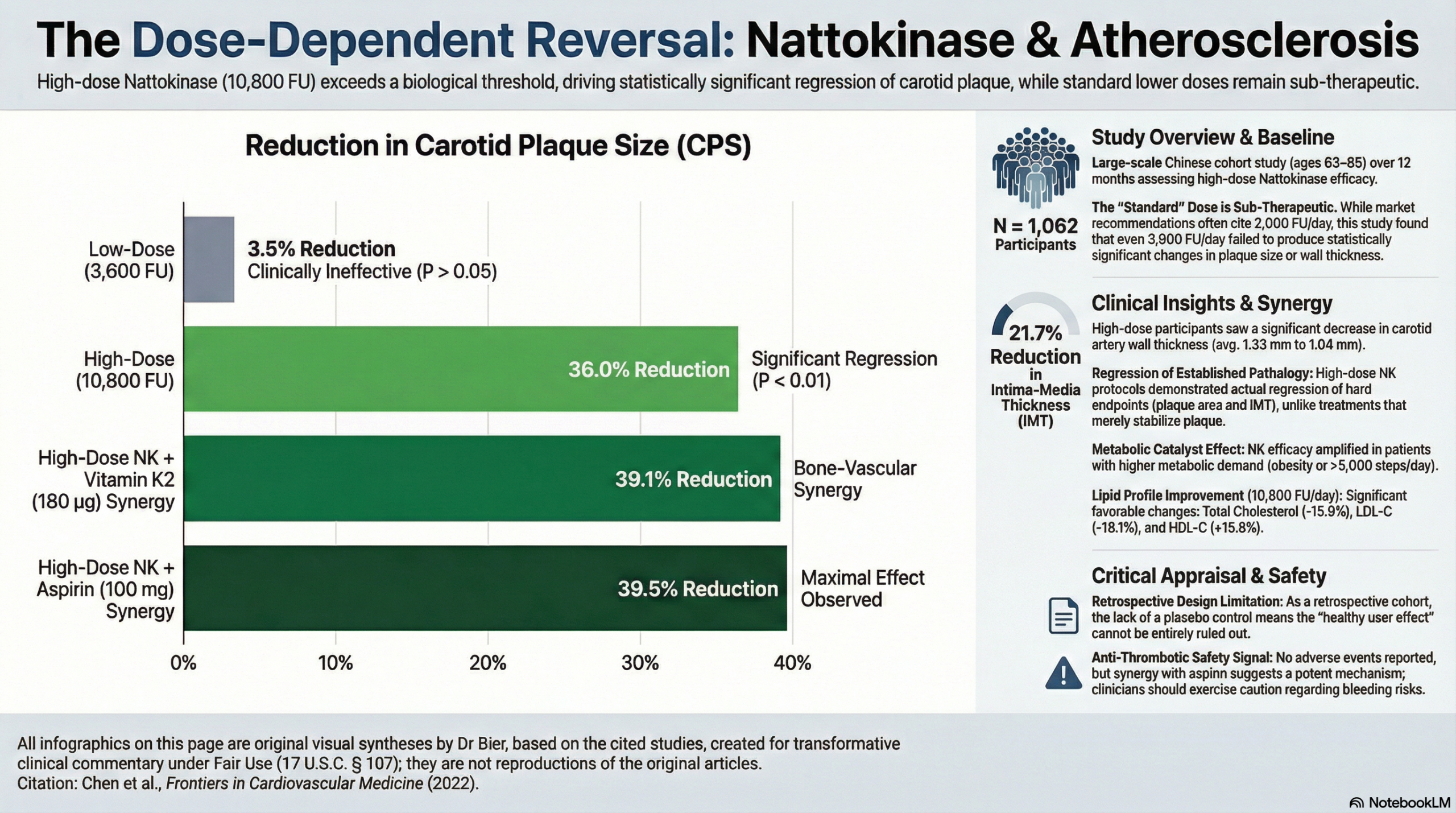
The results in this cohort provide a powerful signal for the potential of natural compounds when applied at therapeutic scales. The striking 36% reduction in carotid plaque size seen with the 10,800 FU dose serves as a definitive takeaway: nattokinase can achieve regression of a hard clinical endpoint provided the dose meets the biological requirement. This is compared to the lower 3,600 FU dose, which the data found was effectively indistinguishable from baseline for plaque reduction.This evidence suggests that standard recommendations may be clinically insufficient when the specific goal is the reversal of atherosclerosis.
Since the objective is the regression of established plaque, low-dose protocols are ineffective and vascular integrity appears to demand a much higher therapeutic ceiling than previously assumed. Based on this the 10,800 FU level should be viewed as the current biological standard for achieving significant carotid remodeling. Additionally, it highlights other potential synergies – the observation that co-administration with Vitamin K2 or Aspirin further enhanced outcomes and that obese participants and those with disciplined exercise habits saw more prominent results indicates that NK may act as a metabolic catalyst that works most effectively in an environment of active physiological demand.
Summary:
Clinical Bottom Line
This large retrospective cohort study suggests that high-dose Nattokinase (NK) at 10,800 FU daily is significantly more effective than the commonly recommended 2,000 FU dose for reducing carotid plaque and improving lipid profiles. The study reported a striking 36% reduction in carotid plaque size and a 21.7% reduction in intima-media thickness over 12 months. While these results are promising and suggest that NK can actively promote the regression of existing atherosclerosis, the findings must be interpreted with caution. As a retrospective analysis, it cannot definitively prove causation, and the absence of a parallel placebo control group for the high-dose intervention means we cannot exclude the influence of unmeasured confounding variables.
Results in Context
Main Results: Plaque Regression and Lipids
- Carotid Plaque Size (CPS): The mean CPS decreased from 24.9 ± 9.8~mm2 to 15.94 ± 7.3~mm2, representing a 36% reduction over 12 months (P < 0.01).
- Intima-Media Thickness (CCA-IMT): The thickness of the carotid artery wall decreased from 1.33 ± 0.81 mm to 1.04 ± 0.56 mm, a 21.7% reduction (P < 0.01).
- Lipid Profile: NK administration led to significant improvements: Total Cholesterol (TC) decreased by 15.9%, Triglycerides (TG) by 15.7%, and LDL-C by 18.1%, while HDL-C increased by 15.8%.
- Improvement Rates: 66.5% of participants showed a reduction in plaque size, and 77.7% showed a reduction in wall thickness.
Definitions
- P-value (P < 0.01): Indicates that there is less than a 1% probability that the observed reduction in plaque size occurred by chance alone.
- CCA-IMT: A measure of the innermost layers of the artery wall; increased thickness is a precursor to plaque formation and a marker of cardiovascular risk.
Participants
- Initial Screen: 2,875 records.
- Final Cohort: 1,062 participants (491 males, 571 females) with hyperlipidemia and/or mild atherosclerosis.
- Plaque Analysis Subgroup: 683 participants had available ultrasound data for plaque and IMT measurement.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Confounding Variables: The study notes that factors like exercise, BMI, smoking, and alcohol consumption influenced the results. While the authors provide subgroup data, the lack of a randomized control group makes it difficult to isolate the effect of NK from these lifestyle factors.
- Dose Response: A major strength is the comparison between 3,600 FU and 10,800 FU, which clearly showed the lower dose was ineffective for plaque regression (3.5% change vs. 36.2% change). This supports a biological gradient, strengthening the association claim.
- Synergistic Effects: The study identified that co-administration with Aspirin (100 mg) or Vitamin K2 (180 µg) further enhanced the lipid-lowering and anti-atherosclerotic effects.
Reporting Quality Assessment (STROBE)
- Confounding Effort: The authors attempted to address confounding by performing subgroup analyses on BMI, exercise, and smoking. However, as a retrospective study, they could not control for these at the outset, and self-reported data (like step counts) could not be validated, which is a major flaw.
- Selection Bias: Participants were from outpatient clinics and community centers; those who were “health conscious” might have been more likely to comply with the 12-month regimen, potentially overstating the effectiveness in a general population.
Applicability
The findings are highly relevant to clinical practice, particularly the suggestion that the standard 2,000 FU dose may be sub-therapeutic for plaque regression. However, the 10,800 FU dose is five times the typical European recommendation, and while no adverse events were reported in this cohort, clinicians should monitor for bleeding risks, especially if co-administered with aspirin.
Research Objective
To examine the efficacy and safety of high-dose Nattokinase (10,800 FU/day) in managing atherosclerosis progression and hyperlipidemia over a 12-month period.
Study Design
A large-scale retrospective cohort study. Ultrasound and blood lipid data were extracted from medical records of participants who had taken NK for 12 months and compared to their baseline values.
Setting and Participants
- Setting: Outpatient clinics and 9 Community Health Service Centers in Guangdong and Yunnan Provinces, China, between 2016 and 2020.
- Eligibility: Subjects with marginal/mild hyperlipidemia or evidence of mild atherosclerosis who completed 12 months of NK at the prescribed dose.
Bibliographic Data
- Title: Effective management of atherosclerosis progress and hyperlipidemia with nattokinase: A clinical study with 1,062 participants
- Authors: Chen H, Chen J, Zhang F, Li Y, Wang R, Zheng Q, Zhang X, Zeng J, Xu F, Lin Y
- Journal: Frontiers in Cardiovascular Medicine
- Year: 2022
- DOI: 10.3389/fcvm.2022.964977
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.