
Comment:
This study reinforces a critical physiological reality often obscured by the aggressive ‘lower is better’ paradigm for lipids. While the cardiovascular benefits of managing dyslipidemia are well-established, we frequently ignore the risks of hypocholesterolemia, such as in this study.
Beyond the diabetes signal identified here, very low LDL (<70 mg/dL) has been consistently linked in other cohorts to increased risks of hemorrhagic stroke and a ‘U-shaped’ all-cause mortality curve—often driven by non-cardiovascular causes such as infection and respiratory disease. This data serves as a crucial reminder that ‘optimal’ does not mean ‘zero.’ For the clinician, a naturally plummeting LDL should not automatically be celebrated as cardioprotective.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
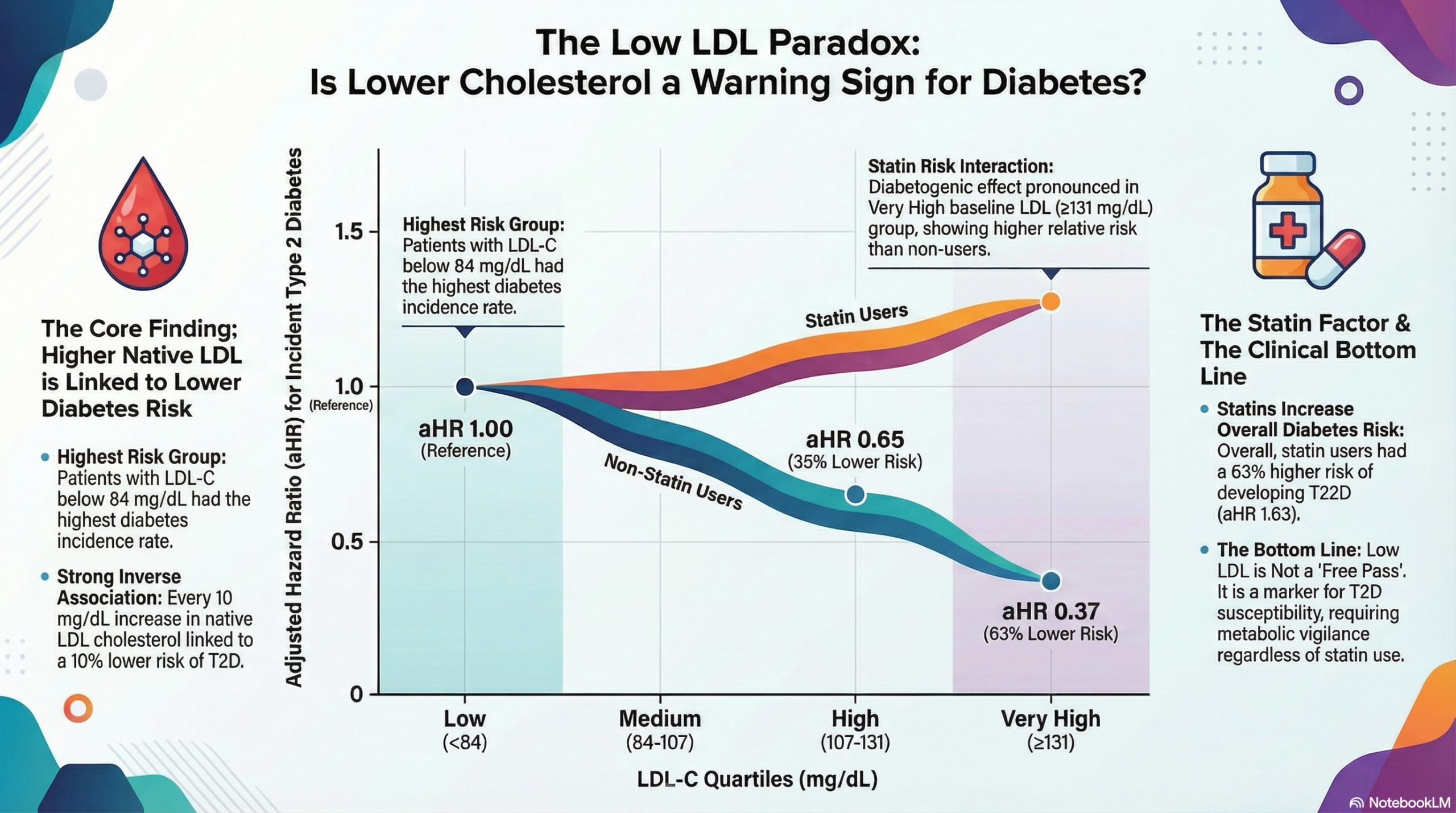
This longitudinal cohort study challenges the prevailing assumption that statin therapy is the sole driver of diabetes risk in dyslipidemic patients. The findings demonstrate a strong, inverse association between native LDL-cholesterol (LDL-C) levels and the risk of incident Type 2 Diabetes (T2D). Specifically, individuals with naturally lower LDL-C (<84 mg/dL) had the highest risk of developing T2D, a phenomenon that appears largely independent of statin use. While statin therapy was associated with an increased risk of T2D overall, the drug-specific risk was most pronounced in patients with very high baseline LDL-C. For the clinician, this suggests that low LDL-C may serve as a biomarker for T2D susceptibility, and that metabolic vigilance is required for patients with low LDL-C, regardless of whether that level is achieved naturally or pharmacologically.
Results in Context
- Main Results:
- Inverse Association: There was a significant inverse association between plasma LDL-C levels and incident T2D (p<0.001).
- Risk by Quartile: Patients in the lowest LDL-C quartile (<84 mg/dL) had the highest risk of developing T2D (27.6 cases per 1,000 person-years) compared to those in the highest quartile (131mg/dL , 8.4 cases per 1,000 person-years).
- Statin Impact: In the overall analysis, statin therapy was associated with a higher risk of T2D (adjusted Hazard Ratio 1.63, 95% CI 1.44–1.84).
- The Interaction: Crucially, when stratified by LDL-C levels, statin therapy significantly increased T2D risk relative to non-users only in the “very high” LDL-C group (131mg/dL ; interaction p=0.018). In the lower LDL-C groups, the risk of T2D was elevated due to the low LDL-C itself, and statin use did not significantly modify this existing risk.
| LDL-C Quartile (mg/dL) | Adjusted Hazard Ratio (aHR) | 95% Confidence Interval | Clinical Interpretation |
| Low (< 84) | 1.00 (Reference) | — | Highest Risk Group (Baseline) |
| Medium (84 – 107) | 0.78 | 0.69 – 0.87 | 22% Lower Risk vs. Low LDL group |
| High (107 – 131) | 0.65 | 0.57 – 0.74 | 35% Lower Risk vs. Low LDL group |
| Very High (≥ 131) | 0.37 | 0.32 – 0.44 | 63% Lower Risk vs. Low LDL group |
Key Takeaway for the Clinician: There is a clear, “dose-dependent” inverse relationship: as native LDL-C increases, the risk of developing new-onset diabetes drops precipitously. Notably, the “Very High” LDL group had less than half the diabetes risk of the “Low” LDL group, independent of other metabolic risk factors.
- Definitions:
- Hazard Ratio (HR): A measure of how often a particular event happens in one group compared to another over time. An HR of 1.63 implies a 63% higher rate of incident T2D in the statin group compared to the non-statin group, after adjustment.
- Inverse Association: As one variable increases (LDL-C), the other decreases (T2D Risk).
The study hypothesizes that intracellular cholesterol uptake plays a role in beta-cell function; understanding the insulin secretion pathway helps visualize where cholesterol homeostasis might interfere.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework):
- Selection Bias (High Attrition): The study started with 202,545 records but analyzed only 13,674 participants. The exclusion of over 90% of the sample due to missing data (specifically BMI and glucose) or exclusion criteria introduces a significant risk of selection bias. The remaining cohort may not be fully representative of the general population.
- Unmeasured Confounding: While the authors adjusted for age, sex, BMI, and hypertension, they lacked data on critical lifestyle factors such as dietary patterns and physical activity. These are potent confounders for T2D risk that could skew the observed associations.
- Lack of Drug Granularity: The study did not have data on statin dosage or potency. This is a major limitation, as the diabetogenic effect of statins is known to be dose-dependent. The authors cannot rule out that the high-LDL group was treated with more intensive statin regimens, driving the interaction effect.
- Reporting Quality Assessment (STROBE):
- The reporting is generally clear, utilizing a real-world primary care database (COMEGEN) which enhances the “real-world” applicability of the findings.
- However, the authors frankly acknowledge that they cannot distinguish whether the low LDL-C is a cause or a consequence (biomarker) of the metabolic state predisposing to diabetes, nor can they elucidate the genetic vs. pharmacologic drivers without genetic data.
- Applicability: The findings are highly relevant to primary care and cardiology, particularly when counseling patients about the metabolic risks of dyslipidemia management. It underscores that “low LDL” is not a metabolic free pass and may flag patients prone to insulin resistance.
Research Objective:
To investigate the relationship between LDL-C plasma concentrations and incident T2D and to evaluate the modifying effect of statin therapy in a large population-based cohort.
Study Design:
- Design: Observational longitudinal cohort study (retrospective analysis of prospectively collected data).
- Data Source: COMEGEN database (General Medicine Cooperative, Naples, Italy).
- Methodology: Cox proportional hazards models were used to evaluate associations, adjusted for baseline characteristics. Interaction terms were used to assess the specific impact of statins across LDL strata.
Setting and Participants:
- Setting: Primary care network in Naples, Italy.
- Participants: 13,674 individuals aged 18–90 years.
- Inclusion Criteria: Free of T2D and cardiovascular disease at baseline; available data on BMI, BP, and biochemistry.
- Cohort Characteristics: 52% were on statin therapy; median follow-up was 71.6 months.
Bibliographic Data:
- Authors: Lembo M, Trimarco V, Pacella D, et al.
- Journal: Cardiovascular Diabetology
- Year: 2025
- DOI: 10.1186/s12933-025-02964-6.
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.