
Comment:
Another in a series of studies that contradicts the dogma that lower cholesterol is better. Although the authors calculated cut off points, using the spline graphs you can see that cholesterol up to about the 230 range is lowest risk of overall deaths and even 300 is better than 160. For cancer you’re safer at even higher levels.
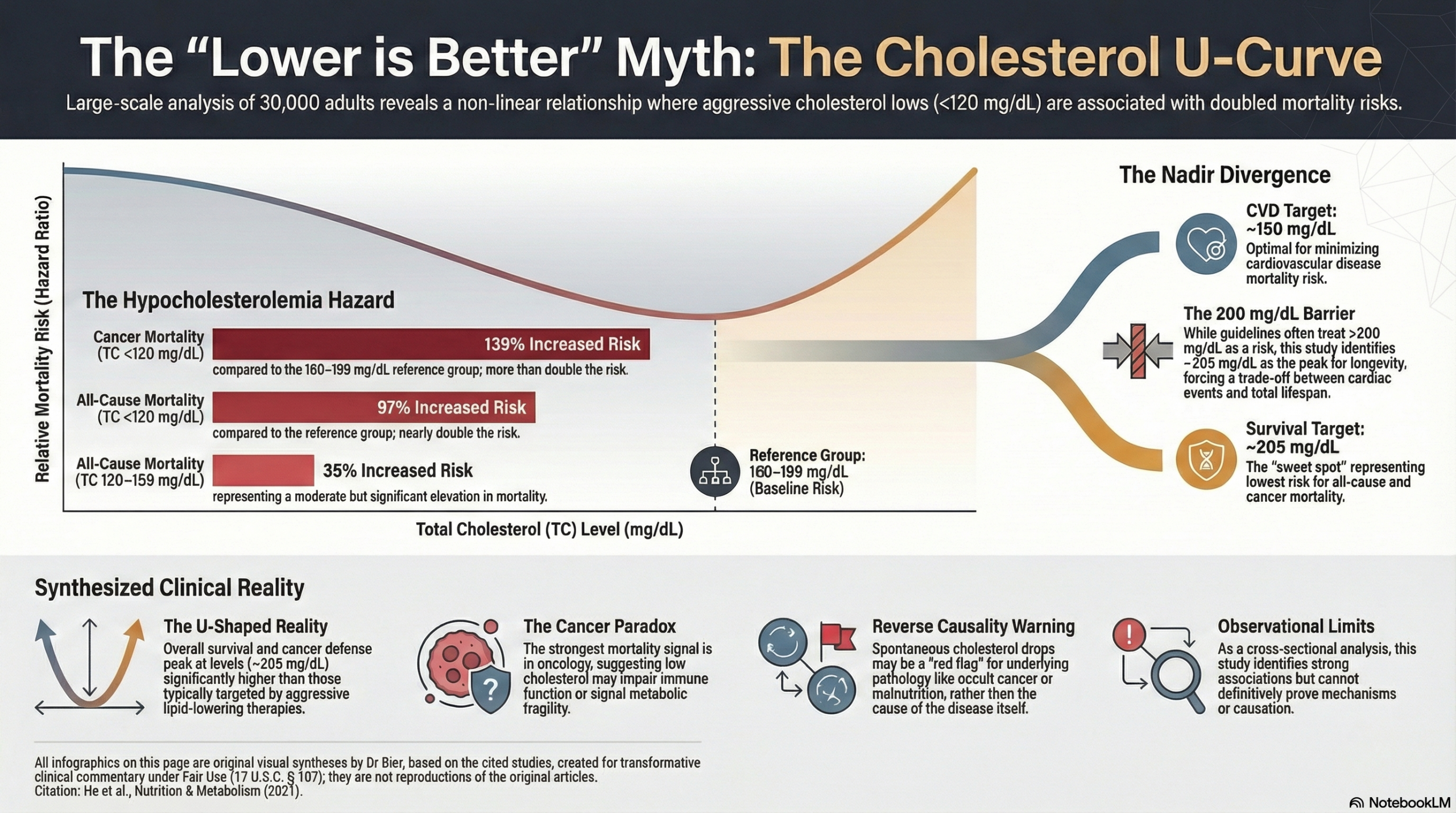
The clinical data on lipid management has reached a point where we must reconcile long-standing biochemical theories with the hard end-point of human survival. For decades, the “lower is better” mantra has defined the standard of care, assuming that driving total cholesterol levels down would linearly extend life. However, this large-scale analysis of over 30,000 adults forces a confrontation with a non-linear biological reality, something we see frequently: the relationship between cholesterol and mortality is a U-shaped curve, not a downward slope.
While extreme low cholesterol levels (specifically <120 mg/dL) are associated with a reduction in cardiovascular risk in isolation, they appear to trigger a devastating signal for systemic health. At these ultra-low levels, individuals faced a nearly doubled risk of all-cause mortality (HR 1.97) and a more than twofold increase in cancer mortality (HR 2.39). This presents a sobering trade-off; an environment intended to be protective for the heart may be inadvertently fostering a significantly higher risk of malignancy and overall death.
Proponents of aggressive lowering often suggest that these findings are the result of “reverse causality”—the hypothesis that subclinical illness causes cholesterol to drop, rather than the low levels causing the illness. While this is a plausible variable to consider, we must treat physiology as the ultimate arbiter. Cholesterol is not a metabolic waste product; it is a vital precursor to steroid hormones and a structural requirement for every cell membrane in the body. When the nadir for cancer survival sits at approximately 205 mg/dL, it suggests that a level traditionally considered “borderline high” may actually be the biological requirement for systemic integrity.
When defining “optimal” cholesterol we need to look at the whole person, not just for cardiovascular risk. The consistent signal linking ultra-low cholesterol to increased cancer and all-cause mortality suggests that we should treat these levels as a potential clinical warning sign rather than a metric of success. The burden of proof rests on aggressive interventions to demonstrate improved Overall Survival, not just a reduction in isolated disease-specific endpoints.
Summary:
This large observational study of over 30,000 U.S. adults found a U-shaped relationship between total cholesterol (TC) and the risk of death, suggesting that both very low and very high levels are associated with increased mortality.
Potential Benefits of “Higher” Cholesterol (Relative to Very Low Levels)
The study’s findings challenge the simple “lower is always better” view for total cholesterol, particularly concerning non-cardiovascular mortality.
-
Lowest All-Cause Mortality Risk: The lowest risk for death from any cause was observed not in the lowest cholesterol group, but in the group with TC levels between 160-199 mg/dL. This group was used as the reference for comparison.
-
Protection Against All-Cause and Cancer Death: Compared to the 160-199 mg/dL range, having very low cholesterol was associated with a significantly higher risk of death. This implies that maintaining cholesterol in a more moderate range (e.g., >160 mg/dL) may be protective against death from cancer and other non-cardiac causes. The optimal TC level for the lowest cardiovascular mortality risk was calculated to be as high as 267 mg/dL, and for cancer mortality, it was 205 mg/dL.
Risks of Total Cholesterol at 200 mg/dL and Lower
While current guidelines often recommend a total cholesterol level below 200 mg/dL to reduce cardiovascular risk, this study highlights potential dangers associated with these lower levels, especially for other diseases.
-
Increased All-Cause Mortality: A total cholesterol level below 200 mg/dL was “strongly linked to a higher risk of death from all causes.”
-
Individuals with TC levels between 120-159 mg/dL had a 35% increased risk of all-cause mortality compared to the reference group (160-199 mg/dL).
-
Those with TC levels <120 mg/dL had a 97% increased risk (nearly double the risk) of all-cause mortality.
-
-
Increased Cancer Mortality: The association was even stronger for cancer-related deaths.
-
Participants with TC levels <120 mg/dL had a 139% increased risk (more than double the risk) of dying from cancer compared to the reference group.
-
-
Important Caveat: The authors suggest that this link between low cholesterol and higher mortality could be due to reverse causality. That is, an undiagnosed underlying illness (like cancer or malnutrition) could be causing cholesterol levels to drop, rather than the low cholesterol itself causing the illness. Therefore, a spontaneous decline in cholesterol may be a marker of a worsening health condition.
Overall Finding from the Spline Graphs
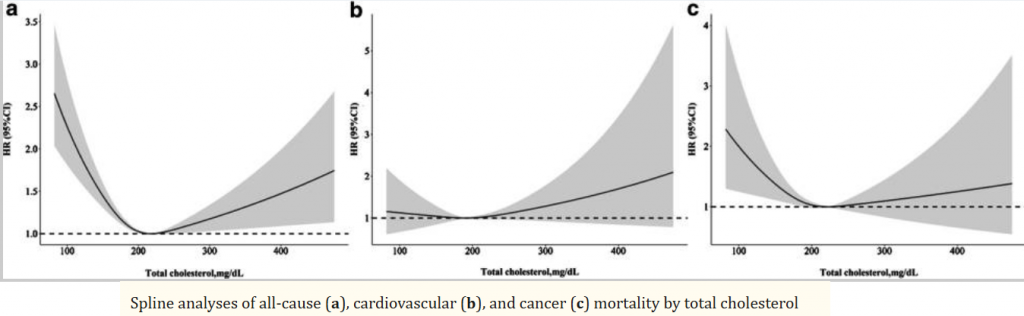
The spline graphs reveal a complex, non-linear (U-shaped) relationship between total cholesterol and mortality. This visual evidence contradicts the simple idea that lower cholesterol is always better, showing that the risk of death increases at both the very low and very high ends of the cholesterol spectrum for different causes.
Graph 1: All-Cause Mortality (Death from Any Cause)
-
Shape of the Curve: The graph shows a distinct U-shape.
-
Interpretation: This indicates that the risk of dying from any cause is lowest at a moderate total cholesterol level. The risk of death significantly increases for individuals with both very low total cholesterol and very high total cholesterol.
-
Lowest Risk Point: The bottom of the “U,” representing the point of lowest mortality risk, occurs at a total cholesterol level of approximately 205 mg/dL.
Graph 2: Cardiovascular Disease (CVD) Mortality
-
Shape of the Curve: This graph shows a more J-shaped or upward-sloping curve.
-
Interpretation: The risk of dying from cardiovascular causes is lowest at lower cholesterol levels and then steadily and significantly increases as total cholesterol levels rise. There is a slight uptick in risk at the very lowest cholesterol levels, but the predominant and most clinically significant trend is the rising risk with higher cholesterol.
-
Lowest Risk Point: The lowest risk is observed around 150 mg/dL, after which the risk consistently climbs.
Graph 3: Cancer Mortality
-
Shape of the Curve: This graph also displays a clear U-shape, similar to the all-cause mortality curve.
-
Interpretation: This visual demonstrates that the risk of dying from cancer is highest at both very low and very high total cholesterol levels.
-
Lowest Risk Point: The nadir of this curve, or the point of lowest cancer mortality risk, is at a total cholesterol level of approximately 205 mg/dL. The increased risk is particularly sharp and significant at cholesterol levels below 160 mg/dL.
Clinical Summary of the Graphs
Visually, the spline graphs provide a powerful summary:
-
For overall survival and cancer survival, a moderate total cholesterol level around 205 mg/dL appears to be optimal. Levels significantly below this are associated with a sharp increase in mortality risk.
-
For cardiovascular health, the traditional view holds, with the risk of death increasing as cholesterol rises, especially above 150-200 mg/dL.
These graphs effectively illustrate the central finding of the paper: the ideal total cholesterol level may depend on the specific health outcome being considered, and very low cholesterol is not without its own risks, particularly concerning cancer mortality.
-
Clinical Bottom Line
This study demonstrates a strong association where total cholesterol levels below 200 mg/dL, and especially below 160 mg/dL, are linked to a significantly higher risk of death from all causes and from cancer. It suggests that the optimal cholesterol level for overall survival may be higher than what is traditionally recommended for preventing heart disease. However, because this is an observational study, it cannot prove causation. Very low cholesterol might be a consequence of underlying disease rather than a cause of it. The findings suggest that while high cholesterol remains a risk factor for cardiovascular death, clinicians should also view very low cholesterol levels as a potential warning sign that warrants further investigation into a patient’s overall health.
Bibliographic Data
-
Title: A nonlinear association of total cholesterol with all-cause and cause-specific mortality
-
Authors: Guo-dong He, Xiao-cong Liu, Lin Liu, Yu-ling Yu, Chao-lei Chen, Jia-yi Huang, Kenneth Lo, Yu-qing Huang and Ying-qing Feng
-
Journal: Nutrition & Metabolism
-
Year: 2021
- DOI: 10.1186/s12986-021-00548-1
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.