
🍵Comment:
Another study dismantling the dogma that coffee is ‘bad for you.’ On the contrary, the data here shows that ‘morning-type’ drinkers enjoy a statistically significant reduction in both all-cause and cardiovascular mortality compared to non-drinkers. These findings also introduce a vital caveat: the circadian context. The fact that heavy consumption is protective only in the morning group suggests that the health benefits are real, but they can be negated by the physiological stress of disrupting sleep cycles with late-day caffeine. It validates coffee as a healthy beverage choice, but one likely best left to the morning hours.
Audio Overview:
Summary:
Clinical Bottom Line
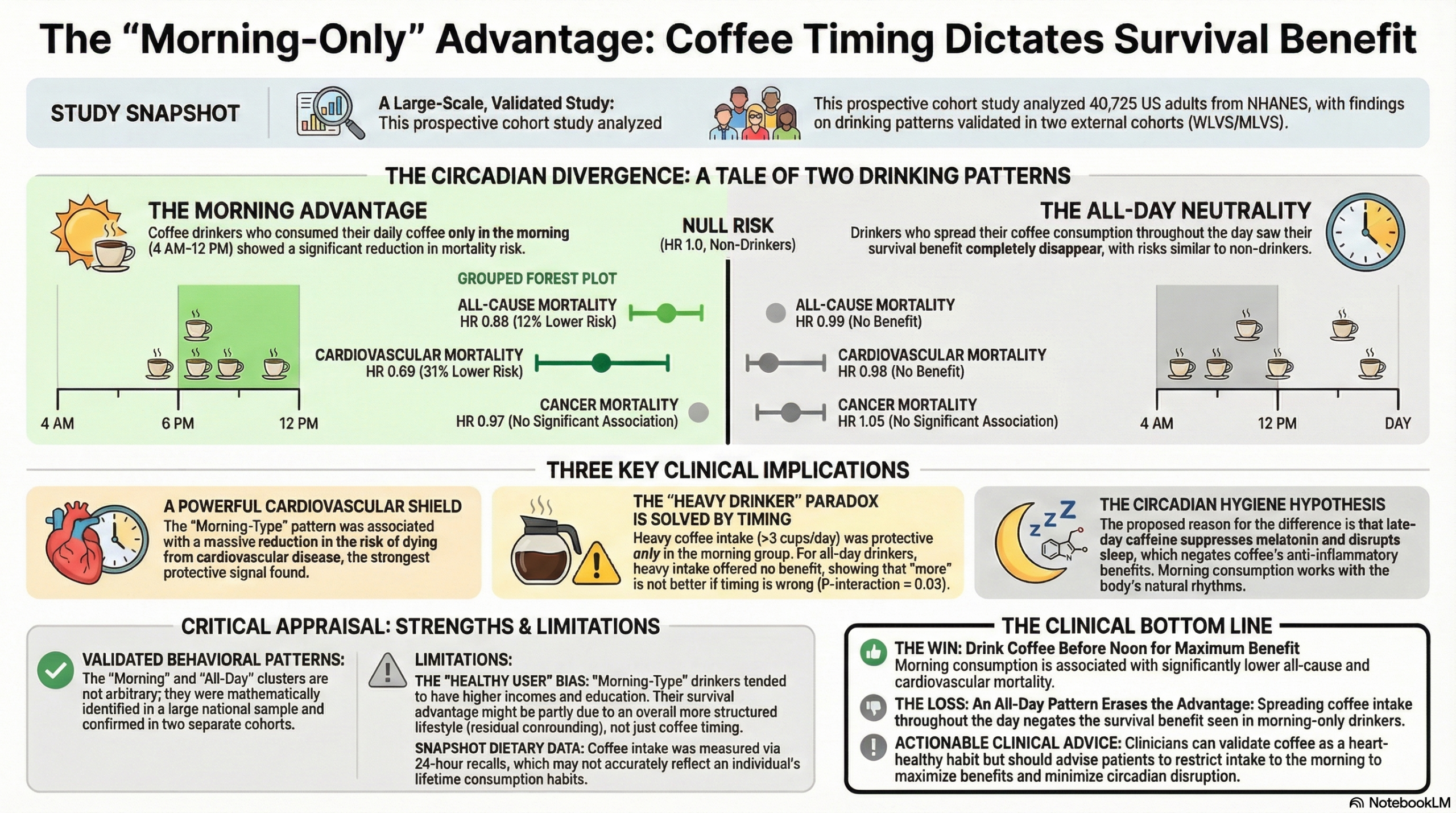
This large observational cohort study suggests that the timing of coffee consumption is a critical variable in its relationship with health outcomes. The analysis found that a “morning-only” coffee drinking pattern is associated with a statistically significant reduction in all-cause and cardiovascular mortality compared to non-drinkers, whereas an “all-day” drinking pattern confers no survival benefit. Furthermore, the study indicates that the often-debated benefit of heavy coffee consumption ($>3$ cups/day) appears restricted solely to those who drink it in the morning. However, as an observational study, these findings cannot prove causation and may be influenced by residual confounding, such as the “healthy user” effect where morning routines correlate with better overall lifestyle hygiene.
Results in Context
-
Main Results (Morning Pattern): Participants categorized as “Morning-type” coffee drinkers had a significantly lower risk of all-cause mortality (Hazard Ratio [HR]: $0.88$; 95% CI: $0.81-0.96$) and cardiovascular disease (CVD) mortality (HR: $0.69$; 95% CI: $0.55-0.87$) compared to non-coffee drinkers.
-
Main Results (All-Day Pattern): Participants with an “All-day-type” pattern showed no significant reduction in risk for all-cause mortality (HR: $0.99$; 95% CI: $0.90-1.10$) or CVD mortality (HR: $0.96$; 95% CI: $0.79-1.16$) compared to non-drinkers.
-
Interaction with Dosage: There was a significant interaction between timing and amount ($P_{interaction} = .031$). Heavy coffee consumption ($>3$ cups/day) was protective against all-cause mortality only in the morning group (HR: $0.79$; 95% CI: $0.65-0.96$), whereas heavy consumption in the all-day group showed no benefit (HR: $0.85$; 95% CI: $0.71-1.02$).
-
Definitions:
-
Hazard Ratio (HR): An HR of 0.69 implies a 31% reduction in the rate of dying from CVD in the morning-coffee group compared to the non-drinking group over the study period.
-
Clustering: The study used a statistical technique to group people based on when they drank coffee, identifying two main distinct behaviors: Morning (4 a.m.–11:59 a.m.) and All-day (spread across morning, afternoon, and evening).
-
-
Participants: The analysis included 40,725 US adults from the NHANES cohort, with patterns validated in two external cohorts (WLVS and MLVS).
Assertive Critical Appraisal
-
Limitations & Bias (STROBE Framework):
-
Measurement Error: Coffee intake was assessed via 24-hour dietary recalls. While the authors validated the patterns in other cohorts, a 24-hour snapshot may not reflect long-term habits, and self-reporting is subject to recall bias.
-
Residual Confounding: This is the most significant threat to validity. Although the authors adjusted for sleep duration, smoking, and diet quality , “Morning-type” drinkers may possess unmeasured characteristics of a structured, healthier lifestyle (e.g., consistent wake times, employment stability) compared to “All-day” drinkers who might rely on caffeine to manage fatigue or shift work.
-
-
Reporting Quality (STROBE): The study adheres well to STROBE guidelines. The authors clearly describe efforts to address confounding and performed extensive sensitivity analyses, including adjustments for tea and soda intake to isolate the coffee effect.
-
Mechanism Plausibility: The authors propose that late-day caffeine disrupts circadian rhythms and melatonin production, potentially negating coffee’s anti-inflammatory benefits. While biologically plausible, this study does not measure melatonin or inflammatory markers directly to confirm this pathway.
-
Applicability: The findings are highly relevant to US general practice but may not generalize to cultures with different social coffee norms (e.g., late-night espresso cultures).
Research Objective
To identify specific patterns of coffee drinking timing in the US population and evaluate their independent and joint associations with all-cause and cause-specific mortality.
Study Design
-
Design: Prospective cohort study using data from the National Health and Nutrition Examination Survey (NHANES).
-
Methodology: Two-step cluster analysis was used to define drinking patterns based on time of day. Cox proportional hazards models were used to estimate mortality risks.
-
Validation: Patterns were internally validated using Day 2 dietary data and externally validated using 7-day dietary records from the Women’s and Men’s Lifestyle Validation Studies.
Setting and Participants
-
Setting: United States (National Health and Nutrition Examination Survey).
-
Participants: 40,725 adults aged 18 or older with complete dietary data, excluding those with history of CVD or cancer at baseline.
-
Follow-up: Median follow-up of 9.8 years, recording 4,295 deaths.
Bibliographic Data
-
Authors: Wang X, Ma H, Sun Q, Li J, Heianza Y, Van Dam RM, Hu FB, Rimm E, Manson JE, Qi L.
-
Journal: European Heart Journal
-
Year: 2025
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.