
Comment:
This study shows interesting nuances, and different than what is often reported about it. It shows a clear ‘ceiling effect’ for iodine toxicity. The jump in subclinical pathology occurs as soon as we leave deficiency, with no significant difference in risk between ‘more than adequate’ and ‘excessive’ intake. Importantly, this toxicity appears strictly subclinical; the lack of variance in overt disease suggests the thyroid can compensate for this excess without losing clinical function, at least in the medium term. Where there may be a difference is in papillary thyroid cancer, which was higher in the excessive intake region.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
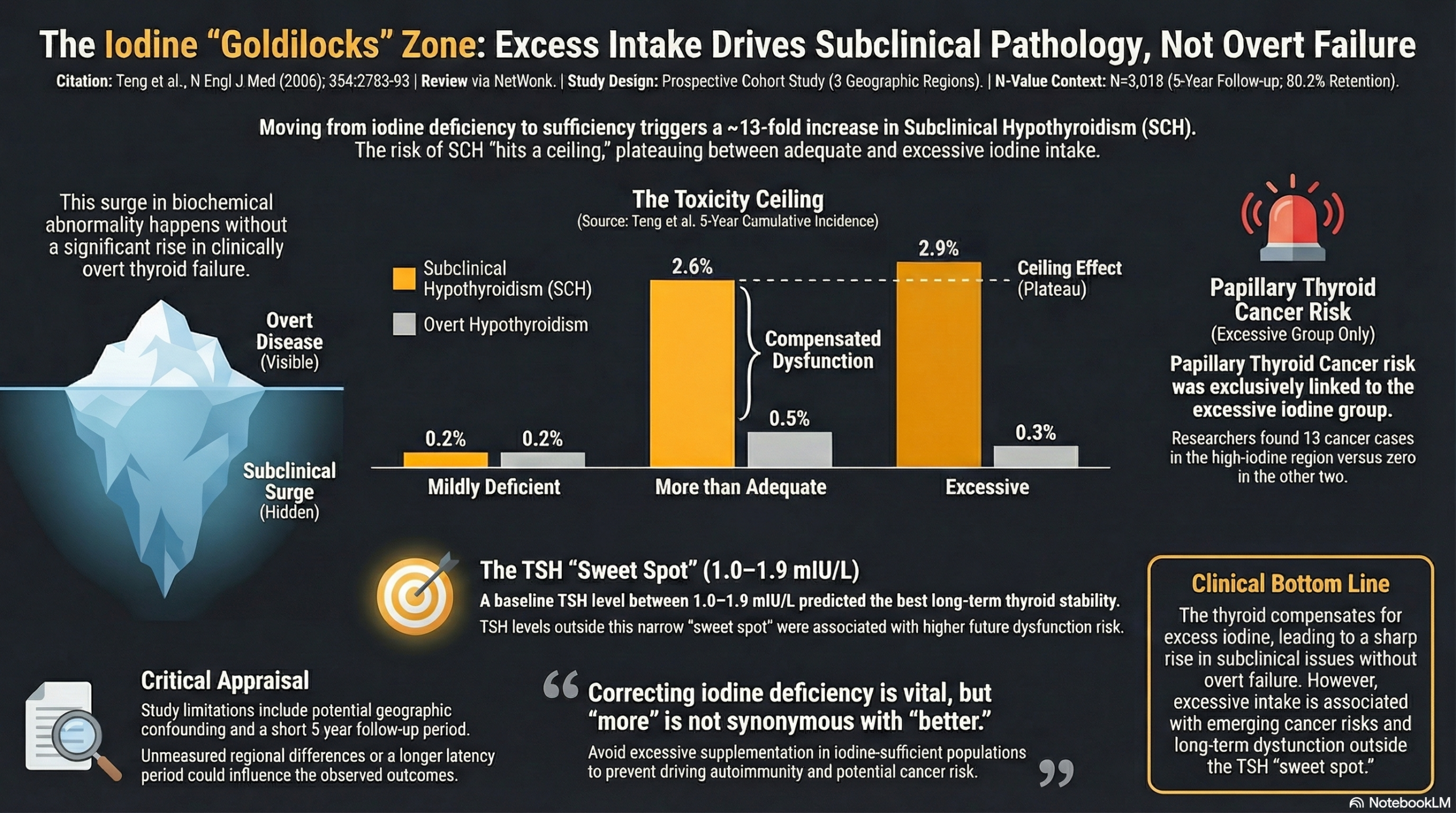
This prospective cohort study demonstrates a complex relationship between iodine intake and thyroid pathology: while iodine deficiency is a known cause of goiter, excessive iodine intake is significantly associated with an increased risk of subclinical hypothyroidism and autoimmune thyroiditis. Importantly, while the study found a strong surge in subclinical disease with higher iodine intake, it did not find a statistically significant difference in the incidence of overt (clinically symptomatic) hypothyroidism or hyperthyroidism over the five-year period.
However, a critical safety signal emerged regarding thyroid cancer, which was exclusively diagnosed in the region with excessive iodine intake. The authors suggest a “U-shaped” relationship for thyroid health, indicating that maintaining iodine intake within a specific “safe” range is critical, and identifying a baseline serum thyrotropin (TSH) level between 1.0 and 1.9 mIU per liter as associated with the lowest subsequent incidence of abnormal thyroid function.
Results in Context
Subclinical vs. Clinically Relevant (Overt) Outcomes
- Subclinical Hypothyroidism (Strong Association): The 5-year cumulative incidence was significantly higher in regions with “more than adequate” and “excessive” iodine intake compared to the “mildly deficient” region.
- Mildly Deficient: 0.2% incidence.
- More than Adequate: 2.6% incidence.
- Excessive: 2.9% incidence.
- Overt Hypothyroidism (No Significant Difference): In contrast to subclinical disease, the cumulative incidence of new overt cases did not differ significantly among the three groups (0.2%, 0.5%, and 0.3%, respectively).
- Thyroid Cancer (Specific Risk): A notable finding was observed regarding papillary thyroid cancer.
- Mild & Adequate Regions: 0 new cases diagnosed.
- Excessive Region: 13 new cases (2 men and 11 women) were diagnosed during the follow-up period.
- Overt Hyperthyroidism & Graves’ Disease: There were no significant differences in the cumulative incidence of overt hyperthyroidism or Graves’ disease among the cohorts.
Additional Key Findings
- Autoimmune Thyroiditis: The incidence rose with iodine intake: 0.2% (deficient) vs. 1.0% (adequate) vs. 1.3% (excessive).
- Goiter: As expected, diffuse goiter was most prevalent in the iodine-deficient region (Panshan). However, the incidence of nodular goiter was significantly higher in the deficient region compared to the adequate region (P=0.03).
- Definitions:
- Subclinical Hypothyroidism: TSH >4.8 mIU/liter with free T4 within the normal range.
- Iodine Levels (Median Urinary Iodine Excretion): Mildly deficient (84 µg/L), More than adequate (243 µg/L), and Excessive (651 µg/L).
- Participants: 3,761 subjects enrolled at baseline; 3,018 (80.2%) completed the follow-up.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework):
- Confounding: The study compares three distinct geographic regions (Panshan, Zhangwu, Huanghua). While the cohorts were similar in age and sex, unmeasured environmental or genetic confounders specific to these regions could influence thyroid autoimmunity independent of iodine intake.
- Latency Period: The authors note that the lack of significant difference in overt hypothyroidism incidence might be due to the relatively short follow-up interval (5 years) relative to the natural history of the disease, suggesting that the surge in subclinical cases might eventually progress to overt disease over a longer period.
- Reporting Quality (STROBE):
- Attrition: The retention rate was 80.2%. While generally acceptable, a ~20% loss to follow-up introduces potential selection bias, though the authors do not explicitly analyze the characteristics of those lost to follow-up compared to completers.
- Statistical Reporting: The authors appropriately used logistic regression to analyze risk factors. Risk factors for developing overt hyperthyroidism included TSH <0.3 mIU/L and presence of goiter.
- Applicability:
- The findings are highly relevant for public health policy regarding salt iodization. They suggest that while correcting deficiency is vital, “more is not always better,” and excessive supplementation in non-deficient populations may drive autoimmune thyroid disease.
Research Objective
To investigate the effect of regional differences in iodine intake on the incidence of thyroid diseases over a five-year follow-up period.
Study Design
- Design: Prospective cohort study with a 5-year follow-up (1999–2004).
- Setting: Three regions in China selected for their naturally different iodine levels:
- Panshan: Mildly deficient (local salt).
- Zhangwu: More than adequate (iodized salt increased intake).
- Huanghua: Excessive (high iodine in drinking water).
Setting and Participants
- Participants: Residents older than 13 years who had lived in the community for more than 10 years.
- Exclusions: Pregnant women and women receiving oral contraceptives.
- Measurements: Urinary iodine, serum thyroid hormones/antibodies, and B-mode ultrasonography were performed at baseline and follow-up.
Bibliographic Data
- Authors: Teng W, Shan Z, Teng X, et al.
- Journal: The New England Journal of Medicine
- Year: 2006
- DOI: 10.1056/NEJMoa054022
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.