
Comment:
This was one of the earlier articles that really helped illustrate how important it is to keep the focus on absolute risk reduction to truly understand how effective an intervention is. Although this is a narrative review and has many risks of bias, other studies have borne out the concerns raised that the absolute reduction benefits of statins is very small.
It also still wins for one of my favorite publication titles.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
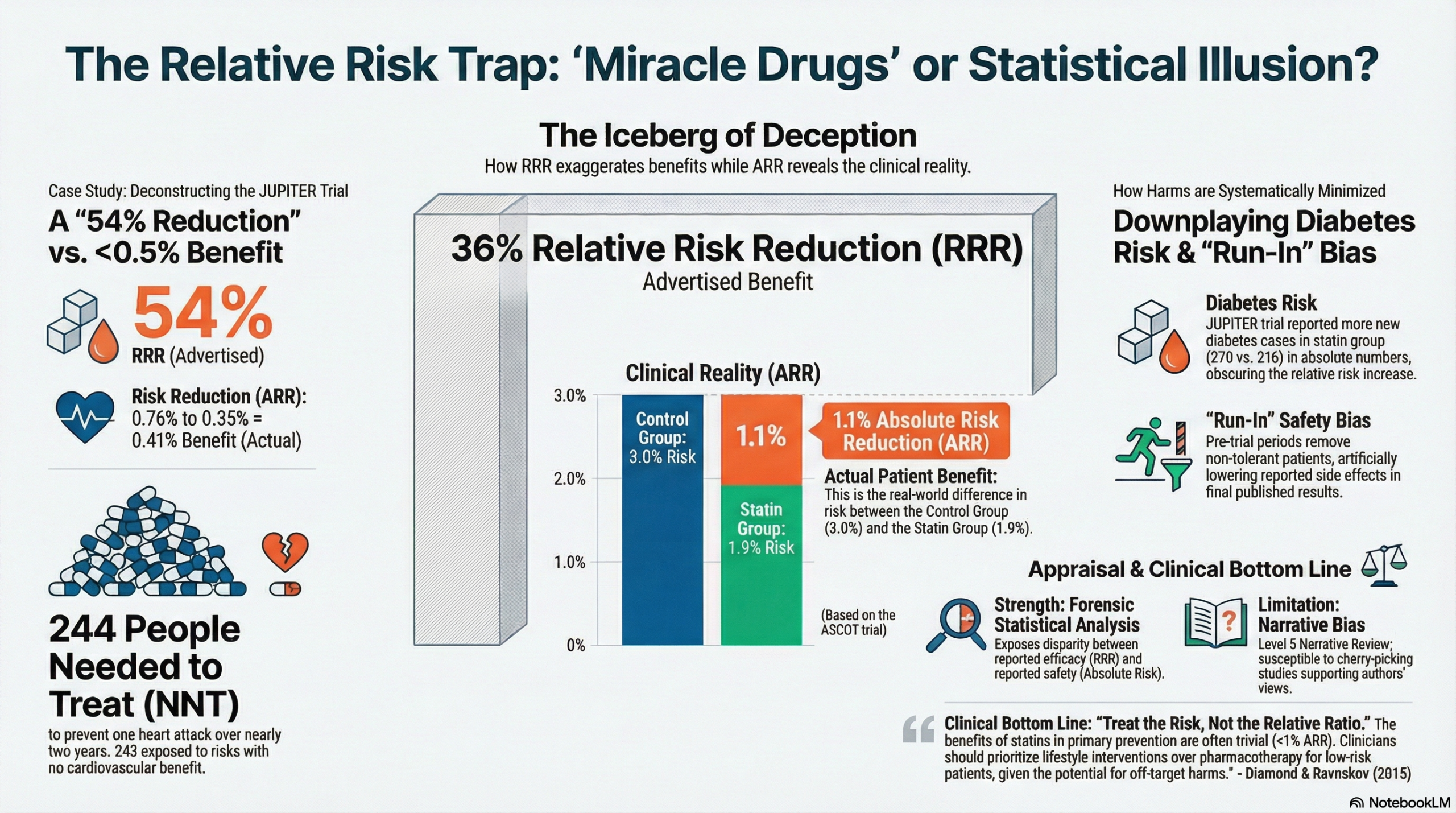
This narrative review argues that the benefits of statins have been systematically exaggerated by pharmaceutical advocates and trial directors through the exclusive use of Relative Risk Reduction (RRR) statistics, while the absolute benefits are trivial (often ≤ 1%). Furthermore, the authors contend that the adverse effects of statins—including cancer, myopathy, and CNS dysfunction—are far more common and serious than reported, often minimized by using Absolute Risk (AR) statistics or excluded via trial run-in periods. The authors suggest that clinicians should focus on lifestyle interventions rather than pharmacotherapy for CVD prevention.
Key Themes & Evidence Summary
- Statistical Deception (RRR vs. ARR): The authors posit that presenting data as RRR amplifies trivial effects. They cite the JUPITER trial, where media reported a “54% reduction” in heart attacks (RRR), while the Absolute Risk Reduction (ARR) was only 0.41 percentage points (0.76% – 0.35%). Similarly, in the ASCOT-LLA trial, a “36% reduction” in fatal CHD/non-fatal MI corresponded to an ARR of only 1.1% (3% vs 1.9%).
- Minimization of Adverse Effects: The review argues that while benefits are inflated via RRR, harms are downplayed using AR or statistical manipulation. For example, in JUPITER, a significant increase in diabetes (270 vs 216 cases) was reported only in absolute terms.
- Run-in Period Bias: The authors highlight that many statin trials (e.g., HPS) utilize a “run-in” period where participants take the drug before the trial officially starts. Those who suffer adverse effects or non-compliance are removed, thereby skewing the safety profile of the final study population.
- Specific Adverse Mechanisms:
- Cancer: The authors cite studies suggesting low cholesterol and statin use are associated with increased cancer risk, noting that trials often exclude skin cancer or are too short to detect long-latency malignancies.
- Myopathy: They argue myopathy rates are underestimated because trials typically only record muscle damage if Creatine Kinase (CK) levels are >10x normal, ignoring symptomatic patients with normal CK.
- CNS/Cognitive: The review cites evidence linking low cholesterol to aggression, suicide, and cognitive impairment, suggesting statins may negatively impact brain function.
Assertive Critical Appraisal
- Evidence Level: Narrative Review (Level 5 Evidence/Expert Opinion). This is a non-systematic presentation of the authors’ perspective and is susceptible to significant selection bias.
- Quality Assessment (SANRA Scale):
-
- Justification & Aims: The aims are clearly formulated: to critique the statistical presentation of statin data.
- Literature Search: Critical Flaw. The authors explicitly state they evaluated findings in a “representative subset” of trial1. There is no description of a systematic search strategy, inclusion criteria, or PRISMA flow. This suggests the authors likely selected studies that supported their pre-existing hypothesis (cherry-picking) while potentially ignoring contradictory high-quality evidence.
- Scientific Reasoning: The argument relies heavily on the discrepancy between RRR and ARR. While accurate that RRR can be misleading, the authors dismiss the clinical significance of small ARRs in preventative medicine without discussing the population-level impact of preventing events in millions of people. Furthermore, they rely on the controversial premise that high cholesterol is not a causal factor in CHD.
- Data Presentation: The comparison of RRR and ARR is presented clearly with specific examples (JUPITER, ASCOT-LLA). However, the critique of adverse events often relies on generating hypotheses (e.g., potential viral mechanisms for cancer) rather than high-level evidence.
- Justification & Aims: The aims are clearly formulated: to critique the statistical presentation of statin data.
Research Objective:
The goal of this review is to explain how “statistical deception” has been used to create the appearance that statins are “wonder drugs,” and to argue that their trivial benefits are outweighed by serious adverse effects.
Bibliographic Data:
- Title: How statistical deception created the appearance that statins are safe and effective in primary and secondary prevention of cardiovascular disease
- Authors: David M Diamond & Uffe Ravnskov
- Journal: Expert Review of Clinical Pharmacology
- Year: 2015
- DOI: 10.1586/17512433.2015.1012494
Mandatory Disclaimer: This AI-generated analysis is for informational and research purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified health provider with any questions you may have regarding a medical condition.
Original Article:
Full text: Not Available
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.