
Comment:
There is a conflict between the biochemical promise of Time-Restricted Eating (TRE) and the hard reality of epidemiological survival data. Protocols like “One Meal a Day” (OMAD) are promoted for their theoretical impact on autophagy and insulin sensitivity, yet frequently ignores the most important metric: Overall Survival. While short-term mechanistic studies suggest metabolic benefit, we must reconcile this with the persistent mortality signals appearing in large-scale human models. Mechanistic plausibility cannot override a mortality signal this strong.
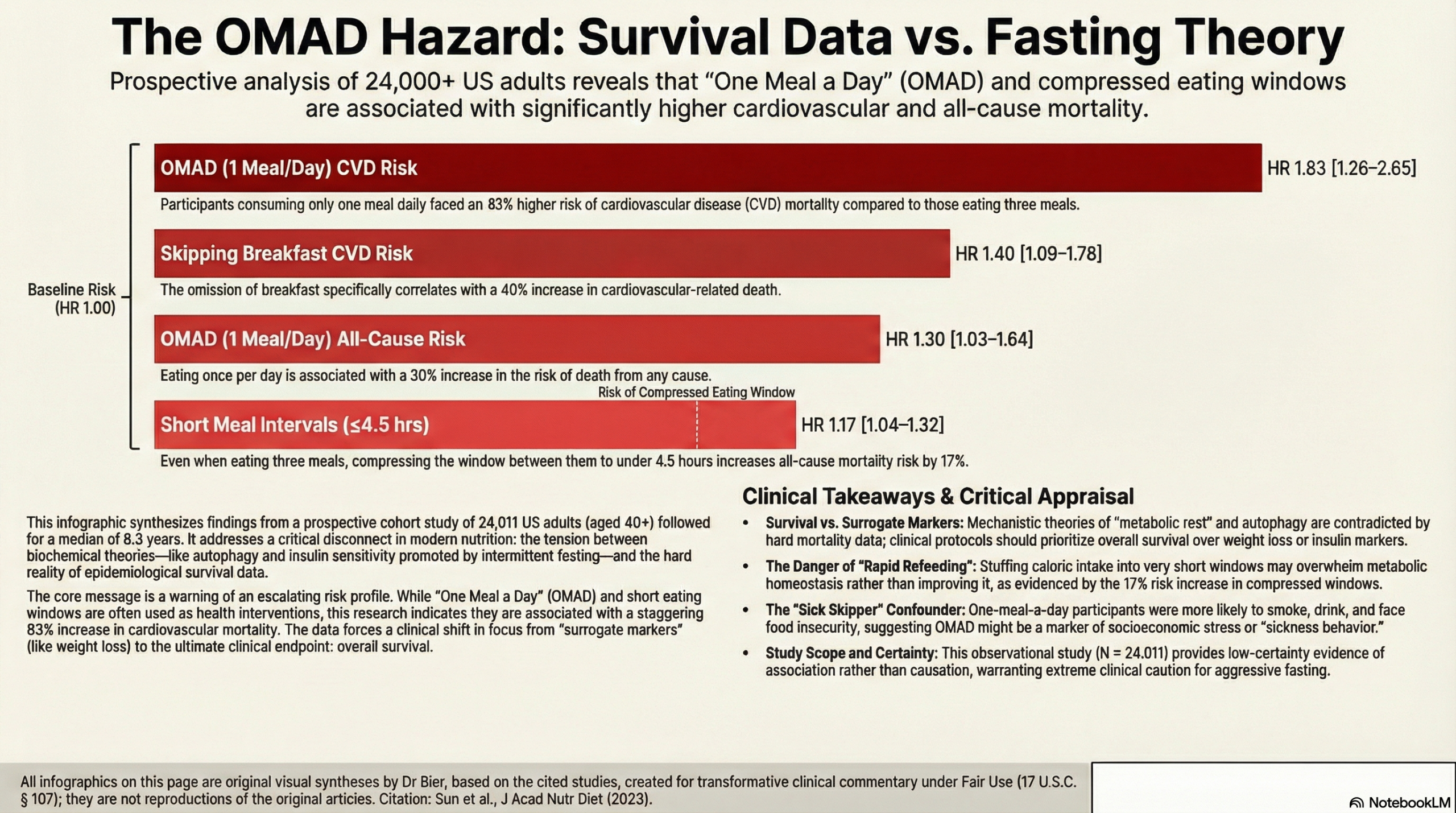
This prospective cohort study of 24,011 US adults disrupts the “fasting is harmless” narrative. By focusing on hard clinical endpoints rather than surrogate markers, the data reveals a distinct, escalating risk profile for restrictive eating patterns:
-
The OMAD Risk: Participants eating only one meal per day faced a significant 30% increase in all-cause mortality (HR 1.30) and a staggering 83% increase in cardiovascular disease (CVD) mortality (HR 1.83) compared to those eating three meals.
Specific Vulnerabilities: The data identifies a specific window of vulnerability; skipping breakfast was associated with a distinct 40% increase in CVD mortality (HR 1.40), whereas skipping lunch or dinner was driven more by all-cause mortality risks.
-
Compressed Windows: Even among those consuming three meals, compressing the eating window (intervals of ≤4.5 hours) was associated with a 17% increase in all-cause mortality (HR 1.17), challenging the safety of rapid re-feeding windows.
Given the magnitude of the cardiovascular risk observed here—particularly the 1.83 Hazard Ratio for those eating once daily—we should treat these aggressive fasting protocols with the same skepticism we apply to pharmaceuticals. The burden of proof lies on the protocol to demonstrate Overall Survival efficacy, rather than relying on surrogate markers like weight loss.
Summary:
Clinical Bottom Line: This prospective cohort study of over 24,000 US adults identifies a strong association between restrictive eating patterns—specifically eating only one meal per day—and significantly increased all-cause and cardiovascular disease (CVD) mortality. Regarding the risks associated with time-restricted eating (TRE) or intermittent fasting (IF) strategies, the data suggests caution: among participants eating three meals daily, a shorter eating interval between meals (≤4.5 hours) was associated with higher all-cause mortality, rather than a benefit. It is crucial to note that while this observational study identifies risk, it cannot prove causation; the “one meal per day” group had higher rates of smoking and food insecurity, raising the possibility that these mortality risks are driven by socioeconomic or behavioral confounders rather than the fasting duration itself.
Results in Context
- Main Results (Risks of Restricted Frequency):
- One Meal Per Day: Compared to participants eating three meals per day, those eating only one meal per day had a Multivariable-adjusted Hazard Ratio (HR) of 1.30 (95% CI 1.03 to 1.64) for all-cause mortality and 1.83 (95% CI 1.26 to 2.65) for CVD mortality.
- Skipping Breakfast: Associated with an adjusted HR of 1.40 (95% CI 1.09 to 1.78) for CVD mortality. * Skipping Lunch or Dinner: Associated with increased all-cause mortality, with HRs of 1.12 (95% CI 1.01 to 1.24) and 1.16 (95% CI 1.02 to 1.32), respectively.
- Short Meal Intervals (Rapid Eating Windows): Among those eating three meals per day, an average interval of \le4.5 hours between adjacent meals was associated with an HR of 1.17 (95% CI 1.04 to 1.32) for all-cause mortality compared to intervals of 4.6 to 5.5 hours.
- Definitions:
- The Hazard Ratio (HR) represents the instantaneous risk of the event (death) occurring in the exposed group (e.g., meal skippers) relative to the reference group (3 meals/day). An HR of 1.83 implies an 83% increase in the risk of CVD death at any given time point.
- Meal Intervals: Calculated as the time between the first and last meal divided by (meal frequency – 1).
- Participants:
- The study included 24,011 adults aged \ge40 years, with 4,175 deaths documented over the follow-up period.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework):
- Residual Confounding and “Sick Skipper” Effect: This is the most critical limitation. Participants eating one meal per day were demographically distinct: they were more likely to be current smokers, heavy alcohol drinkers, food insecure, and have lower diet quality. While the authors adjusted for these factors in Model 2 and 3, observational adjustments may not fully capture the complexity of “sickness behavior” (where ill or socioeconomically stressed individuals skip meals involuntarily), leading to potential reverse causality.
- Exposure Misclassification: Dietary behaviors were assessed using a 24-hour recall. This provides only a snapshot of a single day and assumes it represents long-term habits. It does not distinguish between intentional intermittent fasting for health and unintentional meal skipping due to poverty or lack of appetite.
- Intentionality of Fasting: The authors explicitly note that the study focused on meal skipping regardless of intent; therefore, the evidence regarding the specific “healthy effects” of intentional intermittent fasting regimens is limited. The “one meal a day” group in NHANES likely differs phenotypically from a patient adhering to a structured therapeutic fasting protocol.
- Reporting Quality Assessment (STROBE):
- The reporting is generally robust, with clear definitions of exposure and extensive covariate adjustment. However, the lack of data on sleep duration is a notable omission, as sleep is a potent confounder linking eating patterns and mortality.
- Applicability:
- The findings are highly applicable to the general US adult population aged 40 and older due to the nationally representative sampling of NHANES. However, clinicians should be cautious applying these specific risk estimates to patients practicing structured, nutrition-optimized intermittent fasting, as this study likely captures a broader, less healthy population of “skippers.”
Research Objective: To examine the associations of meal frequency, skipping, and intervals with all-cause and cardiovascular disease (CVD) mortality among US adults.
Study Design: A prospective cohort study utilizing data from the National Health and Nutrition Examination Survey (NHANES) 1999-2014.
Setting and Participants:
- Setting: United States, nationally representative survey.
- Participants: 24,011 adults aged ≥40 years with complete dietary and mortality linkage data. Participants currently pregnant, breastfeeding, or reporting implausible energy intake (<600 or >5000 kcal/day) were excluded.
Bibliographic Data:
- Title: Meal Skipping and Shorter Meal Intervals Are Associated with Increased Risk of All-Cause and Cardiovascular Disease Mortality among US Adults
- Authors: Sun Y, Rong S, Liu B, Du Y, Wu Y, Chen L, Xiao Q, Snetselaar L, Wallace R, Bao W.
- Journal: Journal of the Academy of Nutrition and Dietetics
- Year: 2023
- DOI: https://doi.org/10.1016/j.jand.2022.08.119
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.