
Comment:
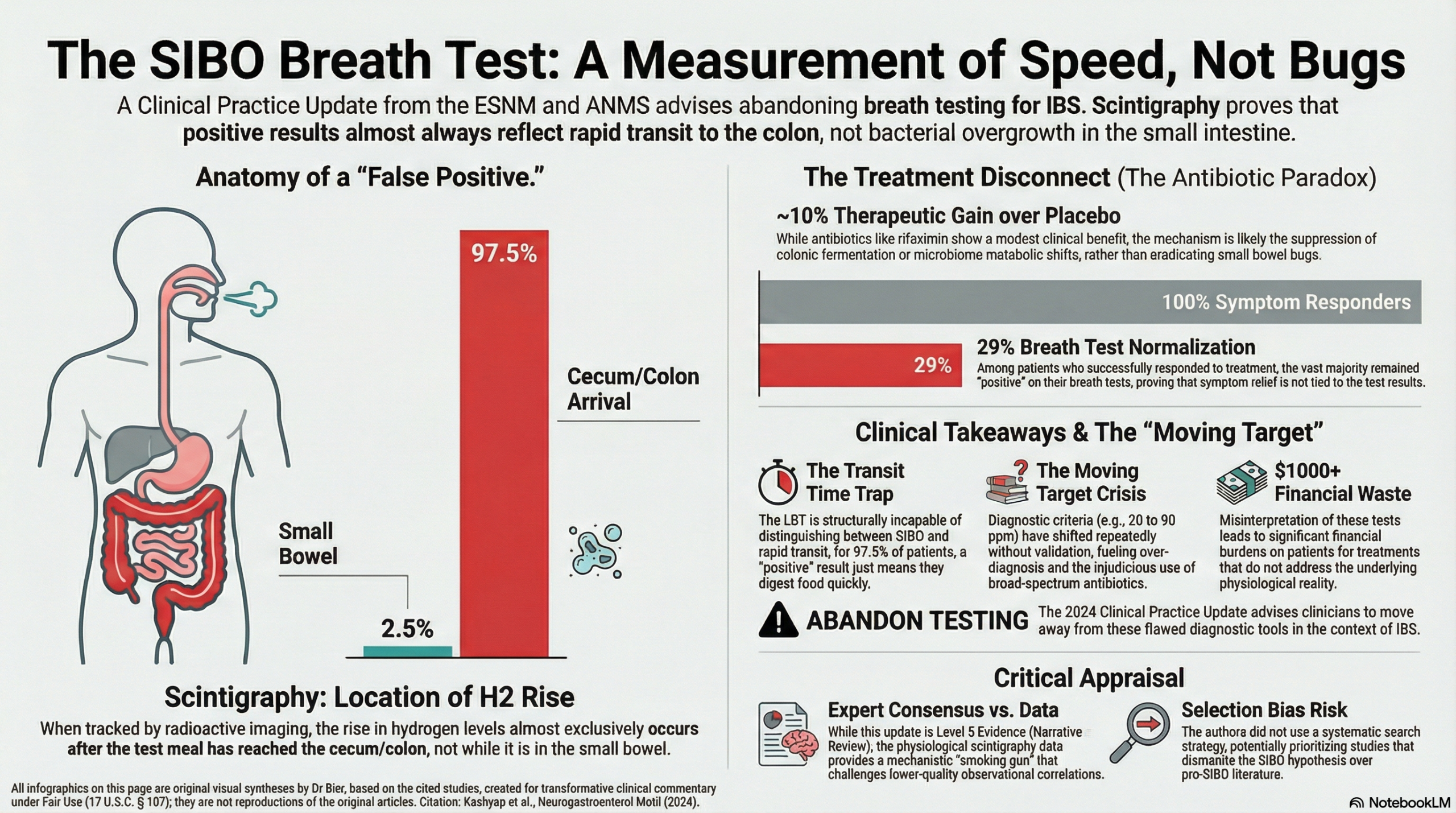
A central issue with the concept of SIB is the conflict between the biochemical allure of a bacterial explanation for complex symptoms and the physiological reality that our diagnostic tools are structurally incapable of distinguishing between overgrowth and simple transit speed. This clinical practice update from the ESNM and ANMS reveals that the Lactulose Breath Test (LBT) is essentially a “moving target” that measures orocecal transit time rather than bacterial density. Scintigraphy confirms that in nearly every case, the rise in H2 occurs only after the test meal has reached the cecum, meaning the test is tracking the speed of a non-absorbable sugar to the colon, not a small intestinal infection. We should recognize that high “SIBO” rates in IBS are likely an iatrogenic artifact of using a test that is naturally positive in patients with rapid transit.
We should be deeply skeptical of the assumption that symptom improvement with antibiotics validates the SIBO hypothesis. The modest 10% therapeutic gain seen with rifaximin in IBS studies likely reflects the suppression of colonic fermentation rather than the eradication of small intestinal overgrowth. Since bloating—the primary symptom improved by these medications—has not been shown to predict SIBO, the conventional narrative that we are “treating the small bowel” is built on a physiological misunderstanding. The definitive takeaway is that a positive breath test in an IBS patient is a non-specific indicator of various GI states rather than a mandate for antibiotic intervention.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This clinical practice update argues that the widespread use of breath testing to diagnose Small Intestinal Bacterial Overgrowth (SIBO) in patients with Irritable Bowel Syndrome (IBS) is scientifically flawed and should be abandoned. The authors contend that the Lactulose Breath Test (LBT) primarily measures orocecal transit time rather than bacterial density, leading to a high rate of false positives—particularly in patients with diarrhea-predominant IBS (IBS-D) who naturally have faster transit. While antibiotics like rifaximin show modest benefit in IBS, this effect may be due to the suppression of colonic fermentation rather than the eradication of small intestinal overgrowth.
Key Themes & Evidence Summary
Scope
The review provides a historical overview of “classical” SIBO (malabsorption due to structural stasis) and critiques the “SIBO-IBS hypothesis” which suggests that increased bacterial numbers in the small intestine cause functional bowel symptoms. It examines the physiological limitations of hydrogen breath tests and the shifting understanding of the small intestinal microbiome .
The Problem with Breath Testing Accuracy
The accuracy of SIBO breath testing is undermined by several fundamental physiological and methodological flaws:
- Lactulose Breath Test (LBT) as a Transit Measure: The LBT was originally designed to measure the time it takes for a substance to travel from the mouth to the cecum (orocecal transit time). Because lactulose is non-absorbable, it eventually reaches the high-density bacterial population of the cecum, where it is fermented into hydrogen (H2).
- The “False Positive” of Rapid Transit: In patients with IBS-D, the transit time to the cecum can be less than 90 minutes. An early rise in hydrogen (often used as a SIBO marker) in these patients frequently reflects fast transit to the colon rather than overgrowth in the small intestine.
- Glucose Breath Test (GBT) Limitations: While glucose is absorbed proximally (reducing some transit-related errors), it still lacks sufficient accuracy in IBS patients. Studies show glucose can also escape into the cecum, and GBT results do not correlate well with bacterial counts from jejunal aspirates in this population.
- Shifting Diagnostic Criteria: Proponents of the SIBO hypothesis have repeatedly changed diagnostic cut-offs for H2 levels and jejunal cultures without proper validation, essentially creating a “moving target” for diagnosis.
Key Arguments
- Lack of Predictive Value: A positive breath test does not reliably predict who will respond to antibiotic therapy. In major clinical trials (TARGET studies), normalization of the breath test occurred in only 29% of responders.
- Non-Specific Indicators: A positive breath test appears to be a non-specific indicator of various gastrointestinal diseases (GERD, dyspepsia, celiac disease) rather than a specific marker for SIBO or IBS.
- Focus on Composition over Density: The authors argue that future research should focus on the composition and function of microbial communities rather than just absolute numbers (density).
Assertive Critical Appraisal
Evidence Level
This document is a Narrative Review (Level 5 Evidence/Expert Opinion). While it represents a “clinical practice update” endorsed by two major neurogastroenterology societies, its conclusions are based on the authors’ synthesis of existing literature rather than new primary data.
Quality Assessment (SANRA Scale)
- Justification & Aims: The review is strongly justified by the “serious unintended consequences” of over-testing and injudicious antibiotic use. The aims are clearly formulated.
- Literature Search: Major Flaw. The authors do not describe a systematic search strategy; the review is susceptible to selection bias as the authors may have selected studies that primarily support their critique of the SIBO hypothesis.
- Scientific Reasoning: The reasoning is robust and grounded in established gastrointestinal physiology. The use of scintigraphy to prove that breath tests measure transit is a particularly compelling piece of evidence cited by the authors.
- Data Presentation: The authors use tables and figures effectively to illustrate the inconsistency in antibiotic response rates and the “moving target” of diagnostic criteria.
Applicability
These findings are highly relevant to general clinicians managing IBS. They suggest that the financial burden (up to $300 for testing and $1000 for antibiotics) and the potential for antibiotic-related harms are not justified by the current evidence for breath-test-guided SIBO treatment in IBS.
Research Objective
To critically examine the validity of the SIBO-IBS hypothesis and the accuracy of breath testing, arguing for a shift toward more mechanistic studies of microbe-host interactions.
Bibliographic Data
- Title: Critical appraisal of the SIBO hypothesis and breath testing: A clinical practice update endorsed by the European society of neurogastroenterology and motility (ESNM) and the American neurogastroenterology and motility society (ANMS)
- Authors: Purna Kashyap, Paul Moayyedi, Eamonn M. M. Quigley, Magnus Simren, Stephen Vanner
- Journal: Neurogastroenterology & Motility
- Year: 2024
- DOI: 10.1111/nmo.14817
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.