
Comment:
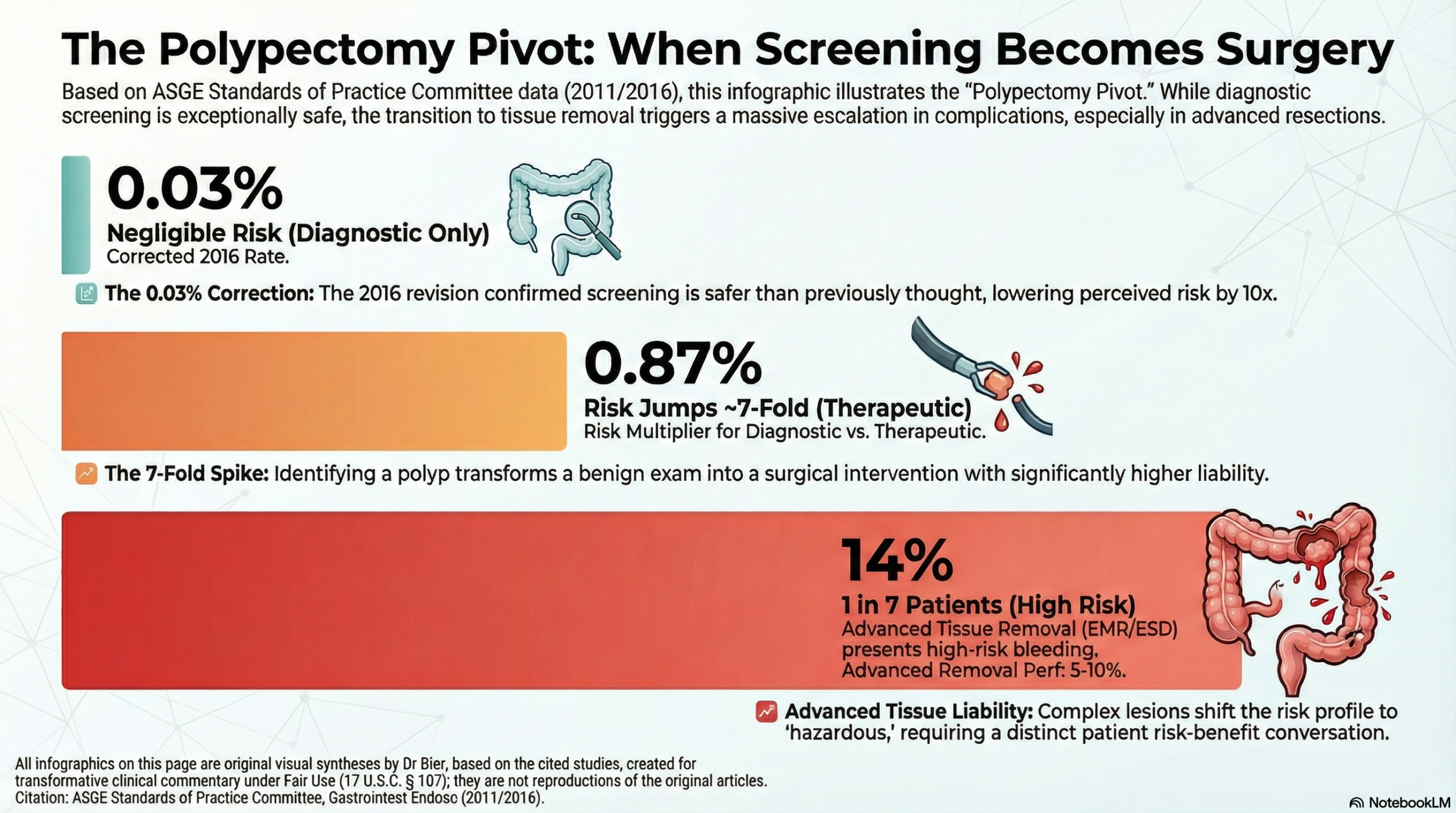
A fundamental conflict exists between the perception of colonoscopy as a “perfectly safe” routine screening and the dramatic iatrogenic escalation that occurs once a procedure becomes therapeutic. While the corrected data for diagnostic perforation is a negligible 0.03%, this “safety halo” disappears the moment a polyp is identified for removal. The human clinical data reveals that for something as common as a polypectomy, serious adverse event rates jump seven-fold, pushing complication risks into the almost 1 in 100 range.
The clinical utility of this ASGE position statement is the clear identification of the “polypectomy pivot” as the primary driver of patient harm. When hemorrhage rates for procedures involving any polypectomy reach 0.87%, we can no longer frame colonoscopy as a consequence-free intervention. This risk profile shifts from “concerning” to “hazardous” as we move into advanced tissue removal; for procedures like Endoscopic Mucosal Resection (EMR) or Endoscopic Submucosal Dissection (ESD), perforation rates can climb as high as 5-10%, with delayed bleeding occurring in up to 14% of cases. The definitive takeaway is that procedural risk is highly dynamic; while the scope itself is remarkably safe, the transition to tissue removal—especially advanced techniques—introduces a substantial survival and morbidity liability that must be carefully considered when evaluating the risk-benefit balance versus other options such as Cologuard Plus.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
In the 2016 erratum to the ASGE guideline, it was specifically the perforation rate that was corrected from 0.3% to 0.03% regarding the large study of 116,000 patients. The mortality/death rate remained consistent with the original report.
Complications of Colonoscopy
Clinical Bottom Line
This position statement from the ASGE provides a comprehensive overview of the risks associated with colonoscopy. While minor, transient symptoms affect up to 33% of patients, serious adverse events remain rare. A critical takeaway is the correction of the perforation rate in a major ambulatory series to 0.03% (down from the originally reported 0.3%), significantly lowering the perceived risk for healthy screening populations. However, the clinical risk remains highly dynamic; there is a dramatic escalation—up to seven-fold—when a procedure transitions from diagnostic to therapeutic (polypectomy).
Results in Context
- Primary Risks: The document identifies perforation, hemorrhage, and cardiopulmonary events as the most significant serious complications.
- Polypectomy Impact: Over 85% of serious complications occur in the context of polypectomy.
- Cardiopulmonary Events: These constitute the majority (67%) of unplanned events, primarily related to sedation rather than the procedural mechanics themselves.
- Definitions:
- Perforation: A full-thickness tear in the colonic wall.
- Postpolypectomy Electrocoagulation Syndrome: A transmural burn causing localized peritonitis symptoms without radiographic evidence of perforation.
Procedural Risk Comparison Table
|
Procedure/Outcome |
Perforation Rate |
Hemorrhage Rate |
Mortality (30-day) |
|
Screening Colonoscopy |
0.03% (Corrected) |
0.21% |
0.007% (procedural) |
|
Diagnostic Colonoscopy |
0.05%–0.08% |
0.37% |
0.07% (all-cause) |
|
With Polypectomy |
0.07% |
0.87% |
Rare / Not stratified |
|
Advanced Tissue Removal (EMR/ESD) |
5-10% |
1.5%–14% |
N/A |
|
Colonic Stent (SEMS) |
3.7%–4.5% |
N/A |
High (due to obstruction) |
Assertive Critical Appraisal
- Evidence Level: This is a Narrative Review/Position Statement (Level 5 Evidence) based on expert consensus. It is susceptible to selection bias as the authors may have prioritized specific studies to support consensus.
- Quality Assessment (SANRA Scale):
- Justification & Aims: High; the document clearly updates the 2003 guidelines to reflect evolving technology like EMR/ESD.
- Literature Search: Weakness identified; the search strategy is not fully described (no specific keywords or full database strings), reducing transparency.
- Scientific Reasoning: Strong; the authors appropriately distinguish between “patient-related” and “procedure-related” risk factors.
- The 0.03% Correction: The erratum is vital. The original 0.3% figure for ambulatory centers was an order of magnitude higher than reality, potentially leading to overestimation of risk in the average-risk screening population.
- Applicability: Findings are highly applicable to general clinical practice, particularly the emphasis on the increased risk associated with right-sided polypectomies and older age (>75).
Research Objective
To provide an updated educational guideline on the frequency and risk factors of colonoscopy complications to assist endoscopists in informed consent and patient selection.
Setting and Participants
The review synthesizes data from multiple sources, including the Clinical Outcomes Research Initiative (CORI) database (over 100,000 procedures) and Medicare claims data.
Bibliographic Data
Title: Complications of colonoscopy
Authors: ASGE Standards of Practice Committee (Fisher DA, Maple JT, et al.)
Journal: Gastrointestinal Endoscopy
Year: 2011 (Erratum published 2016)
DOI: 10.1016/j.gie.2011.07.025 / 10.1016/j.gie.2016.09.020
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.