
Comment:
We have reached a saturation point in the evidence regarding coffee and cardiovascular health. Despite persistent concerns that coffee triggers AF episodes, this analysis of 3,835 patients confirms that these subjective fears do not translate into hard clinical harm. The physiological divergence is stark: while patients worry about palpitations, the data reveals a 23% reduction in MACE and a 21% reduction in death from any cause among moderate daily drinkers. We are over-managing a perceived trigger at the expense of ignoring a potentially protective agent.
Prioritizing hard survival endpoints over mechanistic theories is essential for accurate risk assessment. The 29% reduction in heart failure hospitalizations (HR 0.71) suggests that coffee’s influence on the AF-burdened heart is fundamentally restorative. The dose-response relationship follows a clear U-shaped curve, where moderate intake (2–3 cups) provides the maximal hazard reduction. This reinforces the idea that there is a therapeutic window for caffeine and its associated polyphenols that the standard “avoidance” advice completely misses.
The definitive takeaway is that coffee consumption is not a risk factor to be mitigated, but a habit to be preserved. In an elderly AF population where mortality and heart failure are the primary threats, a daily habit that correlates with such significant hazard reductions should be treated with clinical respect. Clinicians should actively reassure their patients that their morning coffee is likely protecting their heart, not endangering it.
Summary:
Clinical Bottom Line
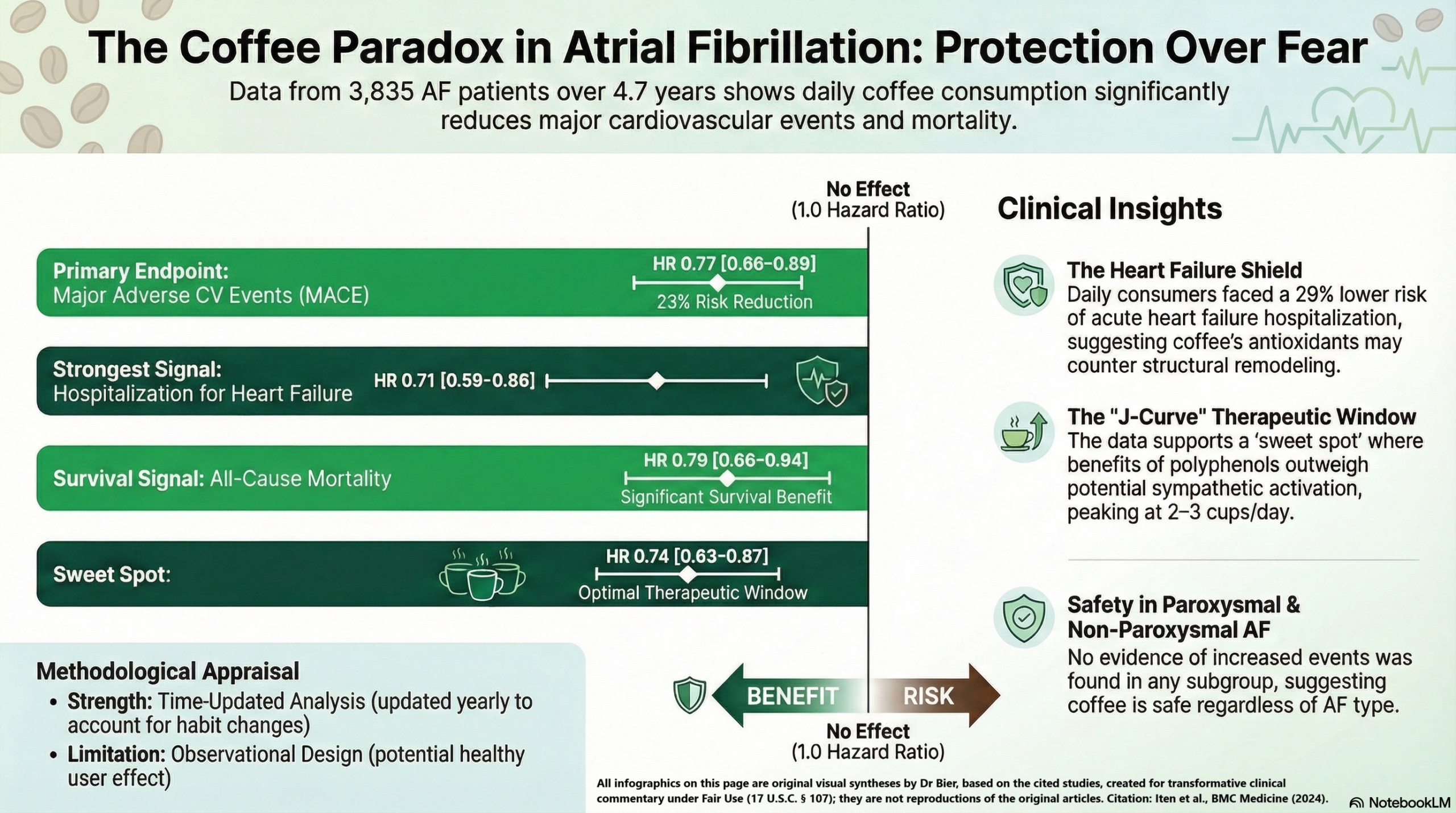
This large, prospective observational study suggests that daily coffee consumption is not harmful—and may actually be protective—for patients with atrial fibrillation (AF). Daily consumption was associated with a 23% reduction in the hazard of major adverse cardiovascular events (MACE), a benefit primarily driven by lower rates of hospitalization for acute heart failure and all-cause mortality. The “sweet spot” appears to be moderate consumption of 2–3 cups per day. While these findings are robust, they are observational; therefore, we can conclude that coffee is safe for AF patients, but we cannot yet definitively state that starting coffee consumption will cause improved cardiac outcomes.
Results in Context
-
Main Results: Daily coffee consumption was associated with a significantly lower risk of MACE compared to not-daily consumption (HR 0.77; 95% CI 0.66–0.89).
-
Definition: A Hazard Ratio (HR) of 0.77 indicates a 23% reduction in the risk of an event occurring at any given time during the follow-up period compared to the reference group.
-
-
Dose-Response (Subcategories):
-
Low (1 cup/day): HR 0.83 (95% CI 0.69–1.00).
-
Moderate (2–3 cups/day): HR 0.74 (95% CI 0.63–0.87), representing the lowest observed hazard.
-
High (≥4 cups/day): HR 0.77 (95% CI 0.60–0.99).
-
-
Secondary Outcomes:
-
Hospitalization for Heart Failure: Strongly reduced in daily consumers (HR 0.71; 95% CI 0.59–0.86).
-
All-Cause Mortality: Significantly lower hazard (HR 0.79; 95% CI 0.66–0.94).
-
Stroke & MI: Results for stroke/systemic embolism (HR 0.75) and myocardial infarction (HR 0.85) showed favorable trends but did not reach statistical significance after full lifestyle adjustment.
-
-
Participants: Out of 3,835 patients analyzed, 80.7% (n=3,095) were daily coffee consumers and 19.3% (n=740) were not-daily consumers.
Assertive Critical Appraisal
-
Limitations & Bias (STROBE Framework):
-
Confounding: While the authors adjusted for a comprehensive set of variables (age, comorbidities, BMI, smoking, and diet), observational studies are always susceptible to “healthy user bias”. It is possible that those who drink coffee have other unmeasured lifestyle habits that contribute to better outcomes.
-
Self-Reporting: Coffee intake was self-assessed via questionnaire, which can lead to misclassification. However, the authors used time-updated data (collected yearly), which is a significant methodological strength as it accounts for changes in habits over time.
-
-
Reporting Quality Assessment (STROBE): The study meets high reporting standards. The authors clearly described their efforts to address confounding by using three progressively adjusted Cox regression models. They also addressed the “competing risk” of non-cardiovascular death, which is vital in an elderly population.
-
Applicability: These findings are highly relevant to general clinical practice. AF patients frequently ask if they should quit coffee due to fears of it being a trigger. This study provides strong evidence to reassure them that moderate consumption is not associated with adverse outcomes and may be beneficial. Note that the population was primarily European, so generalizability to other ethnicities or different regional coffee-making styles remains uncertain.
Research Objective
To investigate the association between coffee consumption and major adverse cardiovascular events (MACE) in a large population of patients with documented atrial fibrillation.
Study Design
Prospective, observational multicenter cohort study. Data were pooled from two Swiss cohorts (Swiss-AF and Beat-AF). Multivariable adjusted time-updated Cox regression analyses were used to determine hazard ratios for clinical outcomes.
Setting and Participants
-
Setting: 14 study centers across Switzerland.
-
Timeline: Enrollment between 2010 and 2017 with yearly follow-up (median 4.7 years).
-
Eligibility: Patients with documented AF. The Swiss-AF cohort primarily included patients aged ≥65 years, while Beat-AF had no age restriction.
Bibliographic Data
-
Title: Coffee consumption and adverse cardiovascular events in patients with atrial fibrillation
-
Authors: Vasco Iten, Elena Herber, Michael Coslovsky, et al.
-
Journal: BMC Medicine
-
Year: 2024
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.