
Comment:
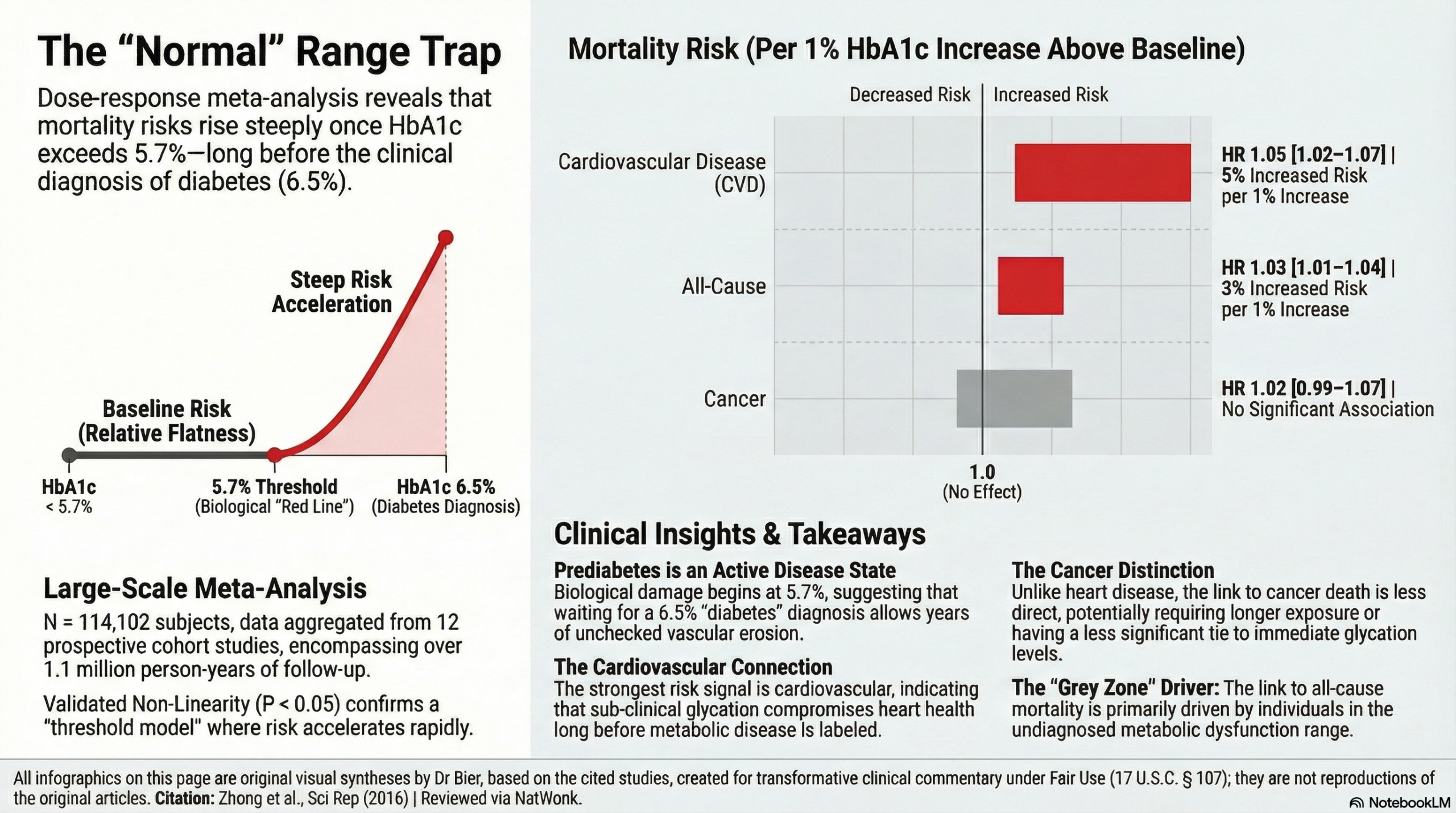
The traditional clinical focus on hemoglobin A1c (HbA1c) often assumes a benign risk profile until the formal 6.5% diabetic threshold is reached, which is something we in the Naturopathic world know to not be true. This dose-response meta-analysis dismantles that assumption, identifying that every 1% increase in HbA1c is associated with a 3% increase in all-cause mortality and a 5% increase in cardiovascular disease (CVD) mortality. It supports that long before we have the official crossover into diabetes, there is damage caused by sub-clinical glycation.
While the dose-response curves were relatively flat below 5.7%, they rose steeply thereafter, indicating that the structural integrity of the vascular system is compromised long before conventional treatments are typically initiated. The data shows that the mortality association is fundamentally driven by those in the undiagnosed diabetes or prediabetes range.
While the association with cancer mortality remained non-significant after excluding undiagnosed diabetes, the risk for cardiovascular death remained persistent and significant. This confirms that the conventional standard-of-care is often too late to address the metabolic requirements of the cardiovascular system. The definitive takeaway for the clinician is that for patients without known diabetes, an HbA1c above 5.7% is not merely a “warning” but an efficacious predictor of mortality risk that necessitates immediate metabolic support to preserve long-term survival.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This meta-analysis suggests that in individuals without a prior diagnosis of diabetes, higher HbA1c levels are significantly associated with increased all-cause and cardiovascular disease (CVD) mortality. However, these associations appear to be primarily driven by individuals who meet the criteria for undiagnosed diabetes (≥ 6.5%) or prediabetes (5.7–6.4%). Regarding cancer mortality, a modest association was observed in the total population, but this became non-significant after excluding those with undiagnosed diabetes. While a “threshold effect” was noted where risks rise steeply above an HbA1c of approximately 5.7%, the findings for cancer mortality specifically are based on a very limited number of studies and should be interpreted with significant caution.
Results
- Summary of Results:
- All-Cause Mortality: Every 1% increase in HbA1c was associated with a 3% increase in the risk of death (HR 1.03; 95% CI 1.01–1.04).
- CVD Mortality: Every 1% increase in HbA1c was associated with a 5% increase in the risk of death (HR 1.05; 95% CI 1.02–1.07).
- Cancer Mortality: The summary HR per 1% increase was 1.02 (95% CI 0.99–1.07), which was not statistically significant in the primary random-effects model.
- Definitions: * Hazard Ratio (HR): A measure of how often a particular event happens in one group compared to another over time; an HR of 1.05 for CVD mortality indicates a 5% relative increase in the hazard of death for every 1% rise in HbA1c.
- 95% Confidence Interval (CI): The range of values within which we are 95% certain the true effect size lies.
Assertive Critical Appraisal
- Certainty of Evidence (GRADE Framework): The evidence is considered Low for cancer mortality and Moderate for all-cause/CVD mortality. The primary reasons for downgrading include:
- Imprecision: The cancer mortality analysis included only 3 studies (36,252 individuals), leading to wide confidence intervals and a potential lack of statistical power to detect a real effect.
- Residual Confounding: As an analysis of observational studies, unmeasured factors (diet, physical activity) may influence both HbA1c and mortality.
- Heterogeneity: * Heterogeneity was low for all-cause (I2 = 28.9%) and CVD mortality (I2 = 4.3%), but moderate for cancer mortality (I2 = 41.2%).
- I2 defined: The percentage of variation across studies due to real differences in study populations or methods rather than chance alone.
- Publication Bias: Assessed via Begg’s and Egger’s tests, which showed no significant evidence of bias (P > 0.1). However, the authors correctly note these tests have low power when only a few studies (like the 3 for cancer) are included.
- Special Consideration for Pooled Results: While the overall pooled result for cancer was non-significant in the preferred random-effects model, it became significant (HR 1.03, 95% CI 1.01–1.06) when using a fixed-effects model. This discrepancy reinforces the need for caution; the finding may be real but is currently obscured by the small number of available studies.
- Reporting Quality Assessment (PRISMA): The study adhered to PRISMA statements and provided a clear flow diagram (Fig. 1) illustrating the selection of 12 studies from an initial 9,956 records.
Research Objective
To clarify the associations and exact dose-response shapes between HbA1c levels and risks of death (all-cause, CVD, and cancer) in subjects without known diabetes.
Study Design
A dose-response meta-analysis of prospective cohort studies.
- Search: PubMed and EMBASE through January 2015.
- Analysis: Two-stage random-effects model and restricted cubic spline functions to assess non-linearity.
Setting and Participants
- Studies: 12 studies (11 cohorts).
- Participants: 114,102 subjects without known diabetes (36.5% men, 63.5% women).
- Follow-up: Total of 1,161,714 person-years with 11,301 recorded deaths.
- Locations: Europe (4), USA (5), and Asia (3).
Bibliographic Data
- Title: HbA1c and Risks of All-Cause and Cause-Specific Death in Subjects without Known Diabetes: A Dose-Response Meta-Analysis of Prospective Cohort Studies
- Authors: Guo-Chao Zhong, Ming-Xin Ye, Jia-Hao Cheng, Yong Zhao & Jian-Ping Gong
- Journal: Scientific Reports
- Year: 2016
- DOI: 10.1038/srep24071
Original Article:
Open Access rights here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.