
Comment:
This review presents a biologically plausible mechanism for why we see such divergent outcomes between dietary omega-3 intake and high-dose pharmacological interventions. While low-to-moderate physiological levels can be antiarrhythmic, the massive dosing used in synthetic pharmaceutical trials may cross a threshold into proarrhythmic territory. The actual clinical utility of this data is the recognition that the iatrogenic signal seen in trials—specifically a 24% increased relative risk of AF—is likely a consequence of these isolated, synthetic formulations rather than a fundamental flaw in the nutrient itself. It highlights a core tension: we cannot equate the metabolic influence of habitual, food-based concentrates with the high-potency, synthetic interventions favored by standard-of-care protocols.
The tangible significance of this synthesis is the confirmation that dose and source are the primary determinants of cardiovascular risk in the omega-3 literature. Dietary intake of approximately 600-750 mg/day is associated with a 12-13% reduction in AF risk, whereas supplemental doses over 1,000 mg/day trigger a dose-dependent increase in that same risk. It is highly probable that the proarrhythmic effect is unique to these high-dose synthetic interventions.
Summary:
Clinical Bottom Line
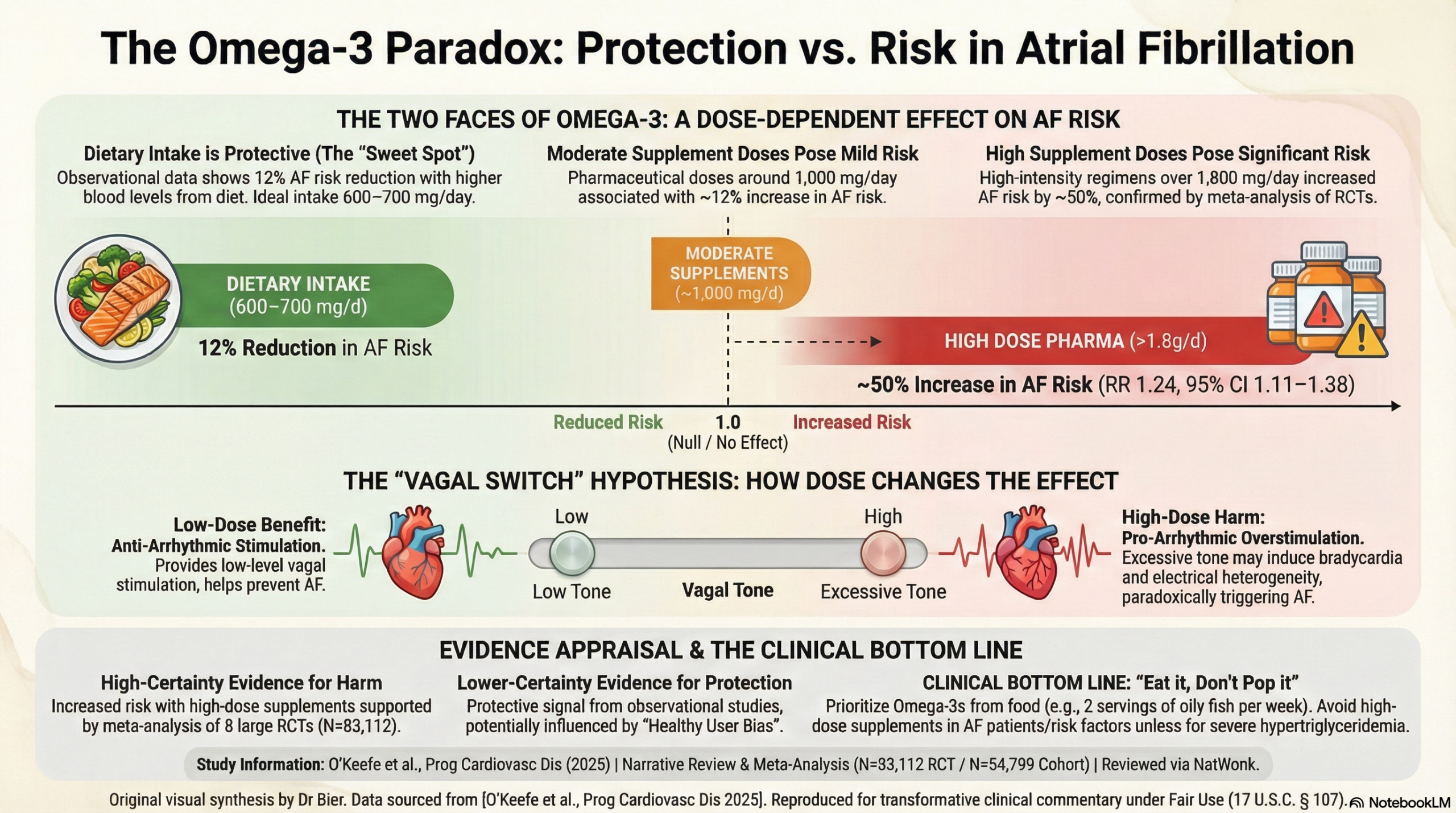
This review presents a compelling “double-edged sword” hypothesis for the effect of omega-3 fatty acids on the risk of atrial fibrillation (AF). The key takeaway is that the dose and source matter. Low-to-moderate dietary intake of omega-3s from fish (around 600–700 mg/day) appears to be associated with a reduced risk of AF. In stark contrast, high-dose pharmaceutical omega-3 supplements (especially those providing over 1,000 mg/day) are associated with a dose-dependent increase in AF risk. The authors propose that this paradoxical effect is mediated by omega-3’s dose-dependent influence on vagal tone.
Results
This review synthesizes findings from randomized controlled trials (RCTs), meta-analyses, and large observational studies, revealing a clear divergence in outcomes based on omega-3 dosage.
-
High-Dose Supplements Increase AF Risk: A meta-analysis of eight large RCTs involving over 83,000 patients found that pharmacologic omega-3 treatment was associated with a 24% increased relative risk of AF (RR 1.24, 95% CI 1.11-1.38). This effect was strongly dose-dependent:
-
Doses around 1,000 mg/day were associated with a modest ~12% increase in AF risk.
-
Doses between 1,800 and 4,000 mg/day were associated with a substantial ~50% increase in AF risk.
-
-
Dietary Intake and Blood Levels Associated with Lower AF Risk: In contrast to trial data on supplements, observational studies suggest a benefit from omega-3s acquired through diet.
-
A pooled analysis of 17 prospective cohort studies found that individuals with the highest blood levels of DHA+EPA had a 12% lower risk of developing AF compared to those with the lowest levels.
-
Dietary studies report a U-shaped relationship, with the maximum risk reduction (around 12-13%) occurring at a daily intake of approximately 630 to 750 mg/day.
-
Assertive Critical Appraisal
This is a narrative review that effectively synthesizes discordant evidence to generate a plausible hypothesis. However, it is not a formal systematic review and lacks the methodological rigor of one (e.g., PRISMA guidelines).
-
Certainty of Evidence: The evidence from multiple large, well-conducted RCTs showing that high-dose omega-3s increase AF risk is of High certainty. The evidence from observational studies suggesting a protective effect of dietary omega-3 is of Low to Moderate certainty due to the inherent risk of confounding (e.g., people who eat more fish may have other healthier lifestyle habits).
-
Heterogeneity: The primary finding of this review is the significant heterogeneity between studies of high-dose supplements and studies of dietary intake. The meta-analysis of RCTs itself showed significant statistical heterogeneity between the low-dose and high-dose trial subgroups (I2=88.8%), strongly supporting the authors’ dose-response hypothesis.
-
The Vagal Tone Hypothesis: The proposed mechanism—that omega-3s increase vagal tone in a dose-dependent manner—is biologically plausible. Low-level vagal stimulation can be antiarrhythmic, whereas high-level stimulation is known to be proarrhythmic and can induce AF. This elegantly explains how low dietary doses might be protective while high supplemental doses become harmful.
-
Conflicts of Interest: It is important to note that several authors have relevant financial disclosures, including roles in companies that sell omega-3 products or offer omega-3 blood testing. While this does not invalidate the findings, it provides important context.
Research Objective
The review aimed to clarify the conflicting effects of marine omega-3 (EPA and DHA) intake on the long-term risk of developing AF and to explore vagal tone as a potential biological mediator for this relationship.
Study Design
The authors conducted a literature search of PubMed to identify and summarize findings from meta-analyses, randomized controlled trials (with at least 500 participants), and prospective observational studies that investigated the link between omega-3s, AF, and autonomic (vagal) tone. The review summarizes data from 8 RCTs and 17 prospective cohort studies, covering tens of thousands of individuals.
Bibliographic Data
-
Title: Omega-3 and Risk of Atrial Fibrillation: Vagally-Mediated Double-Edged Sword
-
Authors: Evan L O’Keefe, James H O’Keefe, Hussam Abuissa, et al.
-
Journal: Progress in Cardiovascular Diseases
-
Year: 2025 (Published online 2024)
Original Article:
Pubmed Central: here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.