
Comment:
This observational MESA study highlights the stark conflict between the idea that early HRT initiation saves lives and the more likely textbook manifestation of healthy user bias impacting outcomes of medical efficacy. Unfortunately the study does not have the data on the formulation used (oral, topical, vaginal), however given the time of intake (2000-2002), it is likely that the vast majority of women were on oral formulations, and therefore these results likely pertain to oral formulations, although we do have other studies showing harm even with the non-oral formulations.
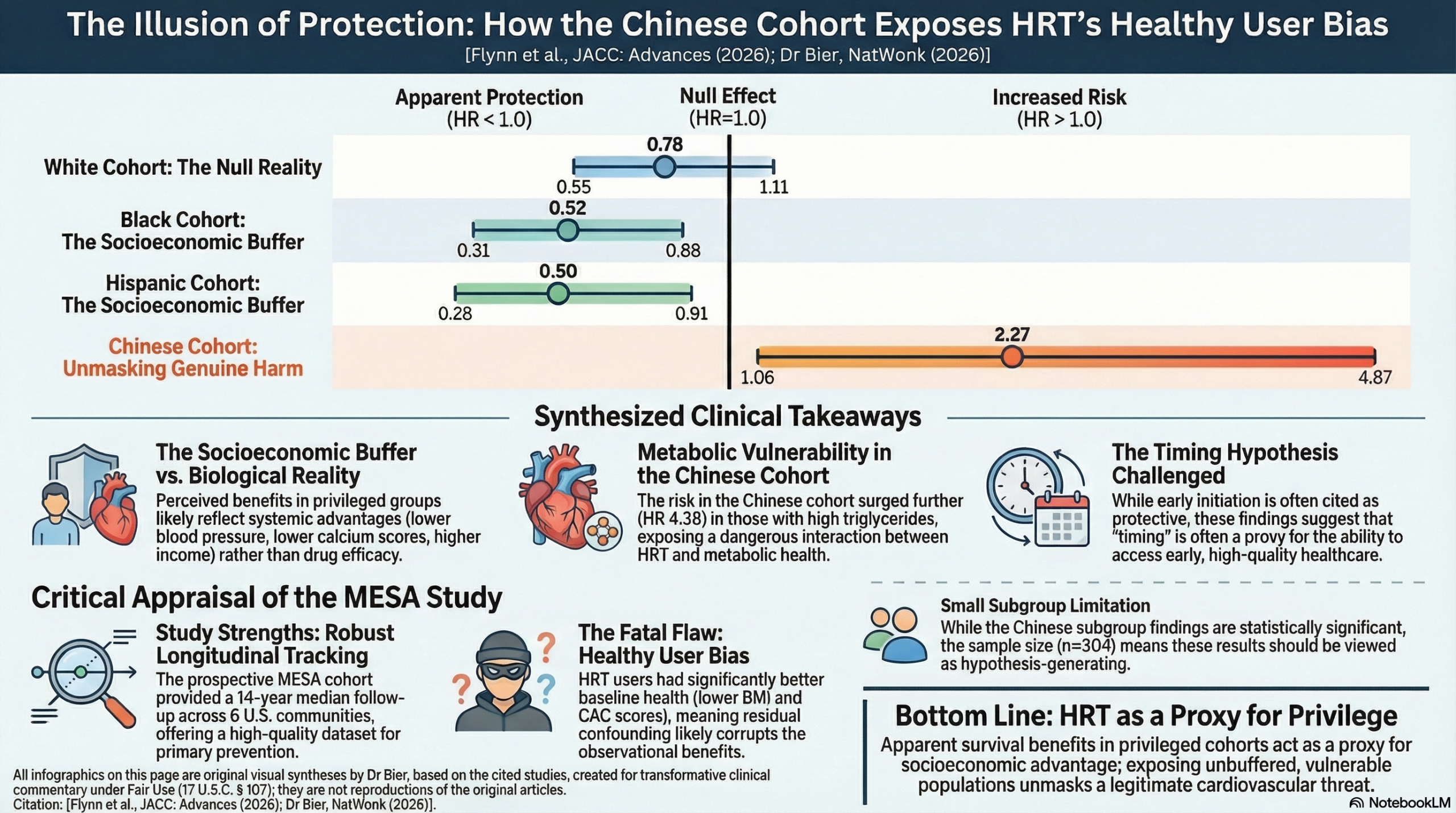
In this study, White women, the reported 35% reduction in overall mortality (HR 0.65) without any corresponding benefit in Major Adverse Cardiovascular Events is a physiological disconnect for a treatment that is purported to improve cardiovascular outcomes, showing the outcome is likely driven by the host’s wealthier baseline demographics, including lower blood pressure and coronary artery calcium scores, rather than the drug. While the benefits seen in Black and Hispanic cohorts (HR 0.52 and HR 0.50 for MACE) suggest protection for those ethnic groups, they more likely represent a “super-healthy” selection filter of women who possessed the high-tier healthcare access required for early initiation. The Chinese cohort provides the corroboration of the bias: they faced a 2.27-fold increased risk of MACE (HR 2.27) that surged to a 4.38-fold hazard in those with high triglycerides (HR 4.38). Unlike the established White, Black and Hispanic cohorts, these women were a 96% foreign-born immigrant population navigating a new medical system without a “wealth buffer” or the same socioeconomic advantages. Healthy User Bias explains the perceived benefits in the White, Black, and Hispanic cohorts as a proxy for socioeconomic privilege—crediting the drug for the survival of women who were already structurally optimized—whereas in the Chinese cohort, the absence of that protective wealth effect allowed the biological interaction between HRT and metabolic vulnerability to reveal the intervention’s more accurate risk profile.
Summary:
Clinical Bottom Line
This analysis of the MESA cohort suggests that hormone replacement therapy (HRT) initiated within 5 years of menopause is associated with a significantly lower risk of major adverse cardiovascular events (MACE) and all-cause mortality across most racial and ethnic groups, providing further support for the “timing hypothesis”. However, a striking and unexpected negative finding emerged: Chinese women on HRT experienced a more than two-fold increase in the risk of MACE. This increased risk was specifically concentrated in Chinese women with the metabolic syndrome or elevated triglycerides. While these results are provocative, they must be interpreted through the lens of a likely “healthy user bias”—as HRT users in this study generally had more favorable baseline health profiles—and the fact that observational data cannot prove that HRT caused these improvements.
Results in Context
Main Results: The Timing Hypothesis In the full cohort, early initiation of HRT (within 5 years of menopause) was associated with a lower risk of both MACE and death:
- All-cause mortality: HR: 0.62 (95% CI: 0.48-0.80, P<0.001).
- MACE: HR: 0.72 (95% CI: 0.55-0.96, P=0.021).
- Definition: A Hazard Ratio (HR) of 0.62 indicates that, at any given time, participants in the early HRT group were 38% less likely to die than those who never used HRT.
Negative Results: Divergence in Chinese Participants The Chinese subgroup was the only one where HRT was associated with worse outcomes:
- Increased MACE Risk: Chinese women on HRT had a 2.27 times higher risk of MACE compared to non-users (95% CI: 1.06-4.87, P=0.035).
- Metabolic Syndrome Interaction: Among Chinese women with the metabolic syndrome, the risk of MACE on HRT was even higher (HR: 3.45, 95% CI: 1.19-9.94).
- Triglyceride Interaction: Chinese women with high triglycerides (\ge150~mg/dL) on HRT faced a four-fold increase in MACE risk (HR: 4.38, 95% CI: 1.14-16.90).
Results by Other Racial/Ethnic Groups (MACE)
- Black Women: HR: 0.52 (95% CI: 0.31-0.88, P=0.014).
- Hispanic Women: HR: 0.50 (95% CI: 0.28-0.91, P=0.021).
- White Women: HR: 0.78 (95% CI: 0.55-1.11, P=0.165).
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Healthy User Bias: This is a critical caveat. Women who were prescribed HRT in this study had significantly better health markers at baseline, including lower BMI, lower systolic blood pressure, lower coronary artery calcium (CAC) scores, and higher income levels compared to non-users. While the authors used multivariate modeling to adjust for these factors, “residual confounding” remains possible—meaning the positive outcomes might be due to the users’ overall healthier lifestyles rather than the HRT itself.
- Lack of Granular Data: The study did not distinguish between different HRT formulations (e.g., oral vs. transdermal) or specific doses, which are known to have different cardiovascular risk profiles.
- Recall Bias: Age of menopause and HRT initiation were self-reported, which may lead to inaccuracies, particularly in older participants.
- Small Chinese Subgroup: While the finding in Chinese women is significant, the sample size was relatively small (n=304 total, 102 on HRT), meaning these results should be viewed as “hypothesis-generating” rather than definitive clinical proof.
Reporting Quality Assessment (STROBE) The authors clearly described their efforts to address confounding through pre-specified Cox models adjusting for age, BMI, smoking, diabetes, hypertension, and LDL levels. They also performed interaction tests for race and metabolic factors, which is a strength of the analysis. However, the inability to track continued HRT use beyond Exam 4 (a median of 4.8 years after baseline) introduces significant “noise” into the long-term follow-up data.
Applicability The MESA cohort is highly diverse and well-characterized, making these findings relevant to a general U.S. clinical population. However, because the study excluded women with pre-existing CVD, these results apply only to primary prevention.
Research Objective
The study aimed to investigate how HRT use and cardiovascular outcomes differ by race and ethnicity, specifically examining the “timing hypothesis” (initiation close to menopause).
Study Design
This was a prospective cohort study using data from the Multi-Ethnic Study of Atherosclerosis (MESA). Participants were followed for a median of 13.9 years.
Setting and Participants
- Participants: 2,427 postmenopausal women without clinically apparent CVD at enrollment.
- Racial/Ethnic Distribution: White (38%), Black (28%), Hispanic (22%), and Chinese (12%).
- Recruitment: 6 United States communities (Baltimore, Chicago, Forsyth County, Los Angeles, Northern Manhattan/Bronx, and St. Paul).
Bibliographic Data
- Title: Hormone Replacement Therapy and Cardiovascular Outcomes by Race and Ethnicity: MESA (Multi-Ethnic Study of Atherosclerosis)
- Authors: Spencer Flynn, Amier Haidar, Icy Liang, Karol Watson, Tamara Horwich, Preethi Srikanthan
- Journal: JACC: Advances
- Year: 2026
- DOI: https://doi.org/10.1016/j.jacadv.2025.102561
- PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.